
Functional Anatomy of Humor: Positive Affect and Chronic Mental Illness
The adaptive value of positive emotions is supported by their evolutionarily early origins. Both spontaneous smiling and laughing have been documented in nonhuman primate species, most commonly as part of social play. 8 – 10 Gervais and Wilson proposed “nonserious social incongruity” as the common factor for the stimuli that elicit spontaneous laughter, which include safe surprise (infants), tickling and physical play (apes, human children), and incongruity-based humor (human adults, signing apes). 10 The authors note that laughter is both a behavioral response and a signal. In their formulation, laughter and humor benefit both the sender and receiver by spreading positive emotions that promote stability, decrease negativity, moderate stress, and strengthen group identity and cohesion.
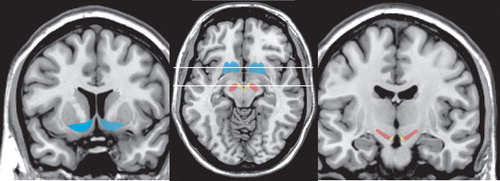
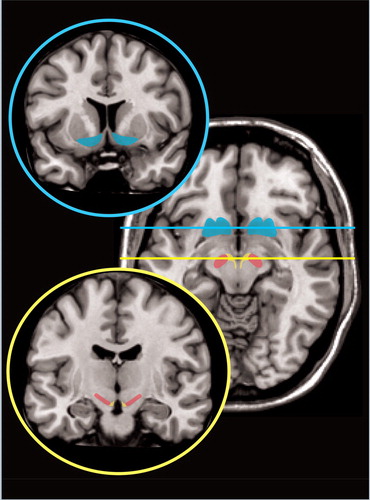
Positive emotions presumably activate areas of the brain involved in reward. 11 The dopamine system is a critical component of the brain reward circuitry, important for motivation, affect and reward-associated functions ( Figure 1 ). 12 – 16 The majority of dopamine-containing neurons reside in two midbrain nuclei, the substantia nigra and the ventral tegmental area (VTA). The dorsal striatum (caudate and putamen) is the major target for the substantia nigra (nigro-striatal projection). The ventral striatum (nucleus accumbens) is a major target for the VTA. The VTA projects to multiple areas of both the cerebral cortex (mesocortical projections) and limbic system (mesolimbic projections).
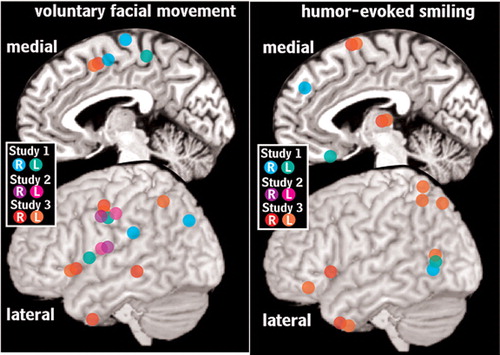
It is important to distinguish true humor-evoked laughter and smiling (Duchenne), which are spontaneous emotionally positive responses, from laughter and smiling that are intentionally generated (non Duchenne). 8 , 10 The neurological pathways involved are clearly different, as indicated by lesion-induced paresis of voluntary facial expression with preservation of emotionally evoked facial expression and vice versa (double-dissociation). 8 Volitional facial paresis has been associated with lesions in primary motor cortex, premotor areas (including the frontal operculum), and/or along the course of the corticobulbar motor tracts. Emotional paresis has been reported in patients with Parkinson’s disease, and has been associated with lesions in the thalamus and striatal structures as well as in the pons (i.e., vicinity of the facial nucleus, CN VII). Recent functional imaging studies have further delineated the cortical areas involved ( Figure 2 ). 1 – 3 Activations (as measured by either positron emission tomography [PET] or functional MRI [fMRI]) were found within primary motor cortex, supplementary motor cortex, and the frontal operculum during voluntary smiling. Primary motor areas were not activated by humor-induced smiling.
Humor is a complex construct, with several stages of processing. Although multiple theories of humor exist, the most accepted is the Incongruity Theory postulated by Sols. 8 , 17 He proposed that humor occurs in two stages. The first involves the listener’s expectation of the joke being disconfirmed by the end; the listener encounters an incongruity (i.e., the punch-line). In the second stage the listener engages in a form of problem solving to resolve the incongruity between the punch-line and the expectation shaped by the joke. This has also been described as “surprise” and “coherence,” a similar formulation to that of “nonserious social incongruity” (see above). A third stage has been proposed: detecting that what actually makes sense is pleasant nonsense (appreciation). 8
Functional imaging provides a way to identify areas of brain involved in different types of humor and stages of processing. A common approach has been to look for areas in which activation correlates with a measure of amusement intensity (funniness). 1 – 5 , 18 , 19 Results can be complex to interpret. Such activations may be due multiple processes including solving the incongruity in order to understand the joke and appreciation of the humor. Results may also be influenced by how the degree of funniness is determined. For example, a study that used the intensity of smiling (as measured by electromyography) found activity correlated with smiling only in medial prefrontal cortex (BA 6) and putamen, both motor-related areas. 1 Studies that have used subject ratings of funniness, on the other hand, have generally found much more widespread activations.
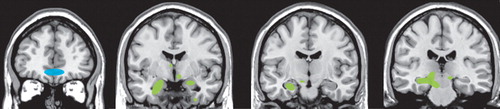
Two studies have used conjunction analysis in order to identify areas of common activation between two types of humor ( Figure 3 ). 4 , 5 One study reported a single area (medial prefrontal cortex, BA 10/11) survived the two step analysis procedure when comparing two types of verbally presented humor (puns and semantic jokes). 4 The other study compared two types of visually presented humor (captioned and uncaptioned cartoons). 5 Multiple regions of activation were found, including posterior temporal cortex, inferior frontal cortex, hippocampus and parahippocampal cortex, amygdala, nucleus accumbens and midbrain.
Given the adaptive value of humor in promoting positive emotions, the brain areas activated during the final stage (appreciation) are of particular interest. 20 One intriguing study has used event-related fMRI during presentation of humorous films (with and without a laugh track) to compare the areas activated just prior to laughter (humor detection) to those active during laughter (humor appreciation). 21 Humor detection was associated with activation in the inferior frontal and posterior temporal cortices for both types of film. Humor appreciation was associated with activation in the insular cortex and amygdala. These results are consistent with previous studies, and support the importance of the posterior temporal and inferior frontal regions in resolving the incongruity. The authors of the study also noted that activation of insular cortex and amygdala is consistent with the visceral and emotional aspects of humor appreciation. The involvement of the amygdala may also relate to its role in memory formation, as humorous material is more easily remembered than material that is not.
Although the beneficial effects of humor and laughter have been part of “common wisdom” for many centuries, there is comparatively little solid scientific research in this potentially quite important area. 22 , 23 As noted above, humor is a complex construct. In research studies humor has been defined in many ways including a stimulus (e.g., viewing a cartoon or humorous film), a response (e.g., laughter), a personality trait (e.g., positive affect), a cognitive process (e.g., resolving the contradiction to understand a joke) and a therapeutic intervention (e.g., humor therapy). The time frame examined has varied from a few minutes to years, depending upon the aspect of humor under investigation. The group sizes range from fewer than 10 individuals to cohorts numbering in the thousands.
Studies that focus on the physiological effects of laughter suggest positive effects on many aspects including immunity and pain tolerance, although some have been criticized on methodological grounds. 22 A more recent review using the broader definition of positive affect (e.g., feelings that reflect a level of pleasurable engagement with the environment) evaluated studies of physical health. 23 The authors differentiated studies of trait positive affect (a stable disposition) and state positive affect (short-term bout), noting that the former would be more likely to influence chronic disease processes, while the latter would be more likely to influence occurrence of sudden events. They found that both prospective and cross-sectional studies support an association between trait positive affect and better health, with lower morbidity in a wide range of conditions (e.g., stroke, accident, common cold). This did not hold for all diseases, particularly those with a high short-term mortality rate (e.g., melanoma). Laboratory studies utilizing induction of state positive affect demonstrated generally positive results (e.g., decreased pain sensitivity/increased pain tolerance, improved immune response). Laboratory studies of the effect on stress responses (as indicated by cortisol level) were less consistent in showing a positive effect. The authors of this review emphasized that there are multiple ways in which positive affect might influence health, some direct (e.g., changes in health practices) and some indirect (e.g., susceptibility to disease, sensitivity to stress).
Humor has been integrated into the practice of medicine in multiple ways. 24 – 26 Perhaps the most common use of humor is to decrease the sense of isolation that is often felt by patients, families, and health care workers. Appropriate use of humor can promote communication and strengthen relationships. Humor must be used with care, however, as poorly timed or ill-chosen humor can be detrimental. Clowns have been used in medicine for about two decades. A recent study compared anxiety levels between children accompanied only by parents and children accompanied by both parents and clowns during the preoperative period prior to minor surgery. 27 The presence of clowns was associated with significantly lower preoperative anxiety, supporting a therapeutic benefit. Interestingly, surveys completed by the medical staff indicated both perception of the benefit to the child and widespread opposition to continuing the program.
Two recent studies have explored the effect of very different humor-centered activities on the behavior of hospitalized psychiatric patients. 28 , 29 In one, twice-weekly clown-lead sessions were provided on an acute psychiatric ward. 28 Sessions were varied, and included games, psychomotor expression exercises and activities based on imaginary situations. Disruptive behaviors during the intervention period were compared to the same period of time (83 days) prior to the intervention. Although there were more patients admitted during intervention period, (101 versus 83) disruptive behaviors decreased in both absolute and relative terms. Of particular interest, the most significantly reduced behaviors were attempted elopements, self-injury and fighting. This change is not likely to be due to differences in the patient populations, as the distribution by diagnosis was quite similar during the two time periods. The authors of the study note that most of the treatment planning in psychiatry is directed toward psychotherapeutic and pharmacotherapeutic inteventions. There has been relatively little focus on the therapeutic milieu. In the second study, movies were provided on two chronic psychiatric wards 5 days per week for 3 months. 29 One group viewed only humorous films. The other group viewed a mixture of film types, with only 15% being humorous. The patients were primarily diagnosed with chronic schizophrenia. A significant reduction in clinically rated negative symptoms, anxiety, and depression was found only in the group that viewed humorous movies. In addition, self-reported anger was decreased and social competence was improved. No changes were found in positive symptoms, activities of daily living, treatment insight, or therapeutic alliance. The authors of the study noted that humorous movies appeared to generate active social exchanges not seen following the nonhumorous (e.g., action adventure) movies. Although these studies must be considered preliminary, they both suggest that humor-based interventions can be quite beneficial to patients with chronic mental illness.
Recently, there has been an increasing emphasis on recovery-oriented care in the treatment of chronic mental illness. A review of research in this area identified multiple mechanisms by which pleasure, play and positive life events help to develop and strengthen a patient’s ability to take an active role in promoting recovery. 30 These insights support the need for further study of the functional anatomy of positive emotions.
1 . Iwase M, Ouchi Y, Okada H, Yokoyama, et al: Neural substrates of human facial expression of pleasant emotion induced by comic films: a PET study. Neuroimage 2002; 17:758–768Google Scholar
2 . Wild B, Erb M, Eyb M, et al: Why are smiles contagious? An fMRI study of the interaction between perception of facial effect and facial movements. Psychiatry Res 2003; 123:17–36Google Scholar
3 . Wild B, Rodden FA, Rapp A, et al: Humor and smiling: cortical regions selective for cognitive, affective, and volitional components. Neurology 2006; 66:887–893Google Scholar
4 . Goel V, Dolan RJ: The functional anatomy of humor: segregating cognitive and affective componenets. Nat Neurosci 2001; 4:237–238Google Scholar
5 . Watson KK, Matthews BJ, Allman JM: Brain activation during sight gags and language-dependent humor. Cereb Cortex 2007; 17:314–324Google Scholar
6 . Burgdorf J, Panksepp J: The neurobiology of positive emotions. Neurosci Biobehav Rev 2006; 30:173–187Google Scholar
7 . Fredrickson BL: What good are positive emotions? Rev Gen Psychol 1998; 2:300–319Google Scholar
8 . Wild B, Rodden FA, Grodd W, et al: Neural correlates of laughter and humour. Brain 2003; 126:2121–2138Google Scholar
9 . Pearce JMS: Some neurological aspects of laughter. Eur Neurol 2004; 52:169–171Google Scholar
10 . Gervais M , Wilson DS: The evolution and functions of laughter and humor: a synthetic approach. Q Rev Biol 2005; 80:395–430Google Scholar
11 . Esch T , Stefano GB: The neurobiology of pleasure, reward processes, addiction and their health implications. Neuro Endocrinol Lett 2004; 25:235–251Google Scholar
12 . Schultz W: Muultiple reward signals in the brain. Nat Rev Neurosci 2000; 1:199–207Google Scholar
13 . Wise RA: Brain reward circuitry: insights from unsensed incentives. Neuron 2002; 36:229–240Google Scholar
14 . Delgado MR: Reward-related responses in the human striatum. Ann N Y Acad Sci 2007; 1104:70–88Google Scholar
15 . Berridge KC: The debate over dopamine’s role in reward: the case for incentive salience. Psychopharmacology (Berl) 2007; 191:391–431Google Scholar
16 . Nicola SM: The nucleus accumbens as part of a basal ganglia action selection ciruit. Psychopharmacology (Berl) 2007; 191:521–550Google Scholar
17 . Suls JA: A two-stage model for the appreciation of jokes and cartoons. in The psychology of humor: theoretical perspectives adn empirical issues, Edited by Goldstein JH , McGhee P. New York, Academic Press 1972, pp 81–100Google Scholar
18 . Mobbs D, Greicius MD, Abdel-Azim E, et al: Humor modulates the mesolimbic reward centers. Neuron 2003; 40:1041–1048Google Scholar
19 . Goldin PR, Hutcherson CA, Ochsner KN, et al: The neural bases of amusement and sadness: a comparison of block contrast and subject-specif emotion intensity regression approaches. Neuroimage 2005; 27:26–36Google Scholar
20 . Berns GS: Something funny happened to reward. Trends Cogn Sci 2004; 8:193–194Google Scholar
21 . Moran JM, Wig GS, Adams RB, et al: Neural correlates of humor detection and appreciation. Neuroimage 2004; 21:1055–1060Google Scholar
22 . Martin RA: Humor, laughter, and physical health: methodological issues and research findings. Psychol Bull 2001; 127:504–519Google Scholar
23 . Pressman SD, Cohen,S: Does positive affect influence health? Psychol Bull 2005; 131:925–971Google Scholar
24 . Rosner F: Therapeutic efficacy of laughter in medicine. Cancer Invest 2002; 20:434–436Google Scholar
25 . Dziegielewski SF, Jacinto GA, Laudadio A, et al: An essential communication tool in therapy. International Journal of Mental Health 2003; 32:74–90Google Scholar
26 . Penson RT, Partridge,RA, Rudd,P, et al: Laughter: the best medicine? Oncologist 2005; 10:651–660Google Scholar
27 . Vagnoli L, Caprilli S, Robiglio A, et al: Clown doctors as a treatment for preoperative anxiety in children: A randomized, prospective study. Pediatrics 2005; 116:e563–e567Google Scholar
28 . Higueras A, Carretero-Dios H, Munoz JP, et al: Effects of a humor-centered activity on disruptive behavior in patients in a general hospital psychiatric ward. Int J Clin Health Psychol 2006; 6:53–64Google Scholar
29 . Gelkopf M, Gonen B, Kurs R, et al: The effect of humorous movies on inpatients with chronic schizophrenia. J Nerv Ment Dis 2006; 194:880–883Google Scholar
30 . Davidson L, Shahar G, Lawless MS, et al: Play, pleasure, and other positive life events: “non-specific” factors in recovery from mental illness? Psychiatry 2006; 69:151–163Google Scholar

