
Electroconvulsive Therapy of a Depressed Patient with Septo-Optic Dysplasia
To the Editor : Septo-optic dysplasia is a syndrome of congenital midline malformations of the forebrain, which is characterized by hypoplasia or absence of the septum pellucidum, hypoplasia or dysplasia of the optic nerves, and pituitary-hypothalamic dysfunction. 1 , 2 Cases of septo-optic dysplasia with other midline structure abnormalities (corpus callosum, fornix), hemispheric lesions (schizencephalic clefts), or pathologic formation of the hippocampus have been reported. 1 Clinical presentations of septo-optic dysplasia include variable ophthalmologic symptoms and endocrine defects. Neurologic impairment and mental retardation are not uncommon. To our knowledge, no psychiatric disorder has ever been reported in septo-optic dysplasia patients. We present a case of major depression with a finding of septo-optic dysplasia by magnetic resonance imaging (MRI) scan as well as treatment response to electroconvulsive therapy (ECT).
Case Report
A 41-year-old man was born without perinatal injury. He had experienced persistent and obvious ataxia since he began to walk and suffered from insomnia, lack of energy, dysphoric mood, social withdrawal, and low-self-esteem since his early teenage years. He did not look for psychiatric help until he was 30 years old. He received at least three kinds of antidepressants with sufficient dosage and duration, 10 sessions of psychotherapy, as well as a single month-long hospitalization, but with limited effect. He had received a third ventriculostomy for hydrocephalus at the age of 39. Postoperative course was unremarkable despite the persistence of ataxia. He was therefore rehospitalized for ECT treatment. On admission, a mental status examination revealed a depressed man with an intact outer appearance. He experienced sleep disturbances and frequent suicidal ideations. Endocrine tests were within normal ranges. MRI of the head revealed hypogenesis of the corpus callosum, agenesis of the septum pellucidum, decreased volume of hippocampus and amygdala, and increased ventricle volume ( Figure 1 ). Hydrocephalus was not likely, based on negative findings of both CSF jet flow study and neurologic examination. No specific abnormality was found in his eyes. The patient received ECT after giving an informed consent. The MECTA SpECTrum 5000Q delivered the stimulus in a bilateral type. Eight successful ECT treatments were performed with a total motor seizure time of 346 sec. Delirium developed transiently after ECT in the first few sessions but was alleviated after the anesthetic agent pentothol was switched to propofol. His memory was mildly impaired but it gradually subsided in time. Mood status was assessed using the Hamilton Depression Rating Scale (HAM-D) at the pre- and 3-month post-ECT (scores of 22 and 23, respectively) did not show responsiveness to ECT. The only improvement was that his suicidal ideation was eliminated when he was discharged.
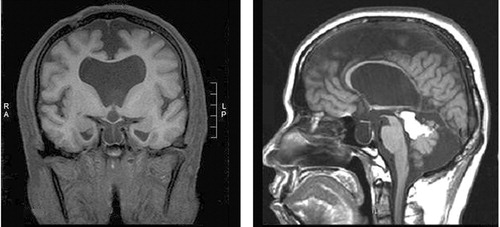
Note: The well formed interhemisphere fissure and hypogenesis of corpus callosum was noted. No septum pellucidum was visualized. The optic chasm was small in size but the pituitary stalk was preserved. The stellar fossa was filling with CSF and the pituitary gland was remarkable decreased in height. The temporal born was dilated on both sides. The hippocampal and amygdala volume were decreased on left side. A lipoma was found in the quadrigeminal.
Comment
We present a case of refractory depression with septo-optic dysplasia who experienced transient delirium and had limited improvement of depressive symptoms in response to ECT. Unlike other septo-optic dysplasia cases, this patient only had depression and ataxia without obvious optic nerve lesions or pituitary-hypothalamic dysfunction. Several studies have found smaller hippocampal volumes in patients with major depression. 3 , 4 We suggest that clinicians should incorporate a differential diagnosis of septo-optic dysplasia in refractory depression patients who were associated with neurological symptoms at early development.
1 . Riedl SW: Auxological, ophthalmological, neurological and MRI findings in 25 Austrian patients with septo-optic dysplasia (SOD): Preliminary data. Horm Res 2002; 58(suppl 3):16–19Google Scholar
2 . Kaplan SL, Grumbach MM, Hoyt F: A syndrome of hypopituitary dwarfism, hypoplasia of optic nerves and malformation of prosencephalon: report of 6 patients. Pediatr Res 1970; 4:480–481Google Scholar
3 . Sheine YI: Depression duration but not age predicts hippocampal volume loss in medically healthy women with recurrent major depression. J Neurosci 1999; 19:5034–5043Google Scholar
4 . Videbech P, Ravnkilde B: Hippocampal volume and depression: a meta-analysis of MRI studies. Am J Psychiatry 2004; 161:1957–1966Google Scholar

