Moral Injury and PTSD: Often Co-Occurring Yet Mechanistically Different
The concept of moral injury has recently emerged in the research literature as a separate aspect of trauma exposure, distinct from posttraumatic stress disorder (PTSD) (15). Moral injury is not classified as a mental disorder. It is a dimensional problem that can have profound effects on critical domains of emotional, psychological, behavioral, social, and spiritual functioning (15–18).
The definitions of moral injury have evolved considerably since its introduction in the 1990s, although a consensus definition has not yet emerged (11, 16, 18–22). The original definition, which was based on work with Vietnam era veterans, focused on failures by leaders. This type of moral injury required that three circumstances be present: “a betrayal of what’s right, by someone who holds legitimate authority, in a high-stakes situation” (20). A later definition of moral injury, which was based on work with Iraq and Afghanistan era veterans, focused on moral failures by the individual (16). This type of moral injury requires that the individual has experienced a potentially injurious event by “perpetrating, failing to prevent, bearing witness to, or learning about acts that transgress deeply held moral beliefs and expectations” and the moral/ethical violation resulted in “lasting psychological, biological, spiritual, behavioral, and social impact” (16). As this definition makes clear, it is important to separate experiencing a potentially morally injurious event from developing moral injury. This is similar to PTSD. Experiencing a trauma (criterion A) does not inevitably lead to developing PTSD. Whether a moral injury develops is determined by how the individual interprets the potentially injurious event. The appraisal process determines whether the event generates significant dissonance with the individual’s belief system and worldview (11, 16, 22–25).
As noted above, the concept of moral injury was initially developed and studied in the context of combat (3, 11, 15, 24–28). There is growing recognition that many of these situations also put civilians (e.g., residents/refugees, journalists, military family members) at risk for moral injury (11, 29–31). In addition, occupations other than military (e.g., first responders, police, health care providers) can include equivalent exposures (11, 29, 30, 32–34). Although much less studied, there are other types of events that are potentially morally injurious (e.g., military/civilian sexual trauma, betrayal by trusted others, homicide/suicide of a loved one, hearing/reading about traumatic events) (29, 30, 35).
The core indications for development of moral injury include self-blame, trust issues, and spiritual/existential issues (11, 21, 36–39). Due to the broad range of possible morally injurious events, many researchers have separated events based on individual responsibility (e.g., perpetration, failing to prevent harm) or other responsibility (e.g., witnessing disproportionate violence, betrayal by trusted others) to better understand the pathological effects of each type (28, 35, 40–42). In general, events involving individual responsibility are more likely to lead to negative internally directed (self-referential) emotions and cognitions (e.g., guilt, shame, lack of self-forgiveness), whereas events involving other responsibility are more likely to lead to negative externally-directed emotions and cognitions (e.g., anger, trust issues, lack of other-forgiveness). Both types of events are associated with spiritual/existential issues (e.g., loss of faith, questioning morality). Until resolved, these internal conflicts can in turn exacerbate social problems (e.g., isolation, aggression, legal issues) and mental health symptoms (e.g., anxiety, depression, PTSD, substance abuse, suicide risk) (43–48).
Moral injury often co-occurs with PTSD, which has been conceptualized as a fear-based disorder. However, studies in military personnel and veterans have found that a significant minority of index traumas for PTSD are events that do not primarily evoke fear/threat (3, 49). A few studies have begun to explore the possibility that the underlying neurobiology of PTSD may be affected by the nature of the index trauma (50–52). A meta-analysis (activation likelihood estimation) of functional MRI (fMRI) studies reported both similarities and differences when studies were grouped by PTSD index trauma type (combat-related, sexual/physical abuse, natural disasters) (1). It is noteworthy that although areas of greater activation were predominately in the right hemisphere for both the combat-related and sexual/physical abuse PTSD groups, there was little or no overlap (Figure 1). One study has compared resting-state regional cerebral metabolic rate between veterans grouped by PTSD index trauma type (danger- and/or fear-based, nondanger-based) as well as to both trauma and civilian controls (2). Regions of interest (ROIs) were brain areas previously reported to be activated by fear stimuli (bilateral amygdala, right rostral anterior cingulate cortex) or by traumatic script imagery (right dorsal anterior cingulate cortex, left posterior cingulate cortex, left precuneus). Veterans with PTSD as a result of danger- and/or fear-based traumas (i.e., life threat to self or other) had higher metabolism in the amygdalae (Figure 1). In contrast, veterans with PTSD due to nondanger-based traumas (i.e., witnessing violence, traumatic loss, moral injury by self or other) had higher metabolism in the precuneus (Figure 1). As noted by the authors, heightened metabolism in the precuneus for nondanger-based traumas may relate to its role in self-referential processing (2).

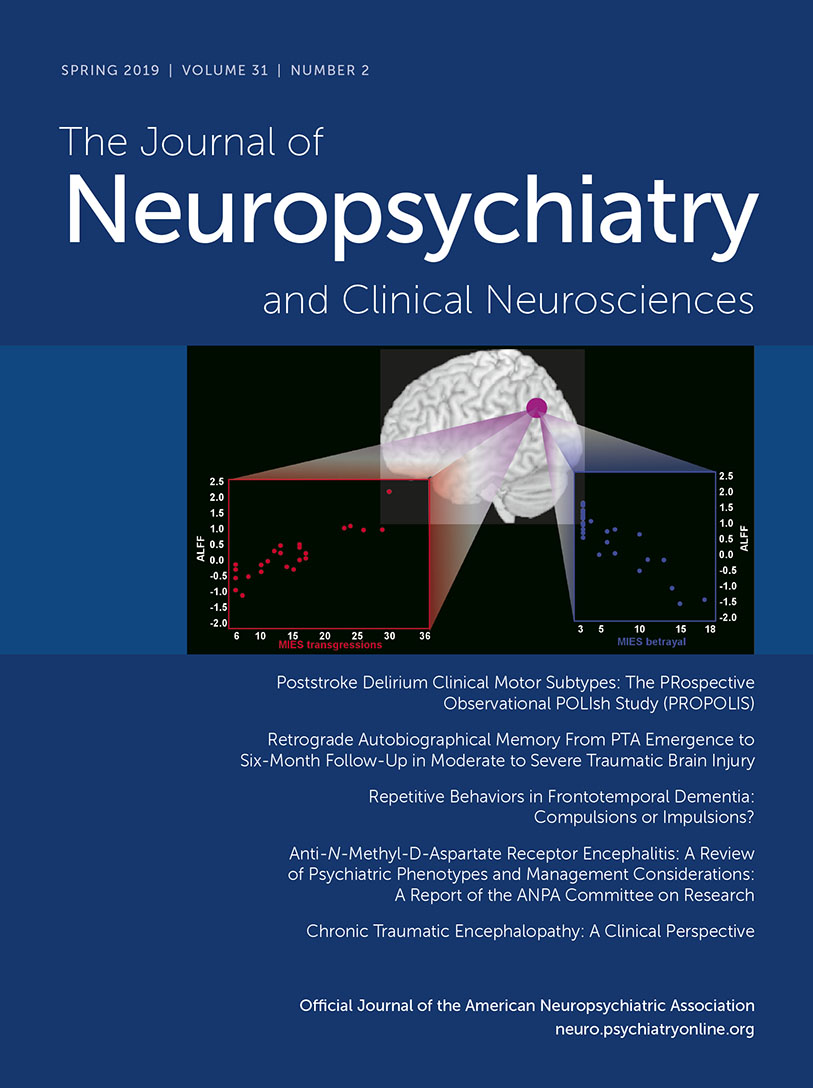
FIGURE 1 and COVER. Recent studies have begun to explore how the underlying neurobiology of posttraumatic stress disorder (PTSD) may be affected by the nature of the index trauma. The results of a meta-analysis that grouped task-activated (trauma reminders) functional MRI (fMRI) studies by PTSD index trauma are color-coded by trauma type (blue, sexual/physical abuse; pink, combat-related) (1). Of note, although areas of greater activation were predominately in the right hemisphere for both groups, there was little or no overlap. One study has compared resting-state regional cerebral metabolic rate between veterans with PTSD grouped by whether the index trauma was danger- and/or fear-based (i.e., life threat to self or other) or nondanger-based (i.e., witnessing violence, traumatic loss, moral injury by self or other). Regions of interest (ROIs) (yellow circles) were areas previously reported to be activated by fear stimuli (bilateral amygdalae, right rostral anterior cingulate cortex) or by traumatic script imagery (right dorsal anterior cingulate cortex, left posterior cingulate cortex, left precuneus). Danger- and/or fear-based traumas were associated with higher metabolism in the amygdala (red fill), whereas nondanger-based traumas were associated with higher metabolism in the precuneus (green fill). As noted by the authors, heightened metabolism in the precuneus for nondanger-based traumas may relate to its role in self-referential processing (2). Moral injury often co-occurs with PTSD. Moral injuries that are index traumas for PTSD are more strongly associated with emotions that developed after the event than emotions experienced during the event, suggesting that the underlying neurobiology may differ (3). An fMRI study of military veterans has explored relationships between resting-state activity (amplitude of low frequency fluctuation [ALFF]) and symptoms of PTSD (Clinician Administered PTSD Scale [CAPS]) and moral injury (Moral Injury Events Scale [MIES]) (4). CAPS score was not significantly correlated with average ALFF in any ROI. Both subscales of the MIES (transgressions, betrayals) correlated with left inferior parietal lobule ROI activity (purple circle) but in opposite directions (Cover). As discussed by the authors, these results indicate that the neural correlates of PTSD and moral injury differ at least in part (4).
Studies of index events for combat-related PTSD have reported that 25–34% resulted in moral injuries (3, 49). Moral injuries differed from index traumas related to life threat as they were more strongly associated with emotions that developed after the event rather than emotions experienced during the event (3). An fMRI study of military veterans has explored relationships between resting-state activity (amplitude of low frequency fluctuation) and symptoms of PTSD (Clinician Administered PTSD Scale [CAPS]) and moral injury (Moral Injury Events Scale [MIES]) (4). Total symptom scores on the CAPS and MIES were not significantly correlated with average amplitude of low frequency fluctuation in any ROI (bilateral amygdale, medial prefrontal cortex, dorsal anterior cingulate cortex, posterior cingulate cortex, inferior parietal lobule). Both subscales of the MIES (transgressions, betrayals) correlated with inferior parietal lobule ROI activity (Figure 1), but in opposite directions (Cover). This was also found in the whole-brain voxel-based analyses. MIES-transgressions was also positively correlated with amplitude of low frequency fluctuation in the fusiform gyrus and posterior insula. In contrast, MIES-betrayals was positively correlated with amplitude of low frequency fluctuation in the precuneus. As discussed by the authors, these results indicate that the neural correlates of PTSD and moral injury differ at least in part (4).
The best treatment for moral injury remains unclear, as most research has focused on alleviating PTSD symptoms. Clinical studies indicate that evidence-based treatments for PTSD (prolonged exposure therapy and cognitive processing therapy) provide some reductions in symptoms (e.g., guilt, shame) arising from coexisting moral injury (10, 11). As noted in both reviews, the focus on identifying trauma-related beliefs and cognitions that are at least partially inaccurate (e.g., exaggerated, distorted, erroneous) as targets for interventions is the likely mechanism. Consistent with this interpretation, a study in veterans reported that the ability to make meaning of a possible trauma by reconciling the discrepancies between one’s belief system and situational appraisal of the event appears to be vital in decreasing the risk for mental health symptoms (43). Similarly, a study of cognitive processing therapy for PTSD due to military sexual trauma reported that reductions in self-blame (but not negative cognitions about self or world) preceded and predicted reductions in PTSD symptoms (53). A recent set of case examples supports efficacy of prolonged exposure therapy and cognitive processing therapy for treating PTSD due to moral injury, provided the index trauma is correctly identified (54).
Others have modified existing treatments to better address the combination of PTSD and moral injury (55–58). A group treating traumatized refugees combined loving kindness mediation with cognitive processing therapy to promote development of positive emotional states (56). A group treating veterans incorporated a spiritual component into cognitive processing therapy to address aspects of moral healing (e.g., spiritual struggles, repentance, forgiveness) (57, 58). Both approaches look promising based on the example cases provided. Adaptive disclosure, which was developed for treating active duty military, combines techniques from cognitive processing therapy with relatively brief exposure therapy (emotion-focused imaginal exposure coupled with meaning making and cognitive restructuring) to address events involving life-threat, traumatic loss or moral injury (55). A randomized clinical trial of adaptive disclosure combined with loving kindness mediation is presently being conducted in veterans (59). Pilot studies also support the usefulness of mindfulness-based therapies (i.e., mindfulness-based stress reduction, loving kindness mediation, mantram repetition) as adjuncts to usual care in veterans and civilians with PTSD (56, 60–64). Beneficial effects included increasing positive emotions, self-acceptance, emotional flexibility, and emotional regulation skills.
Several treatment approaches designed specifically to promote healing from moral injury have been developed, and preliminary studies suggest value (11, 65). One challenge is recognition that in some cases the patient’s beliefs and judgements about their experiences are factually correct (9, 10, 66). Thus, acknowledgment of the past moral/ethical violations (i.e., opening up) may be essential to begin the healing process (9–11). A small study of veterans in a residential PTSD treatment program supports the potential of addressing moral injury in a group setting using acceptance and commitment therapy (67). A pilot study of a cognitive-behavioral therapy module addressing the moral and spiritual impacts of killing reported both acceptability and positive treatment effects (68). It is noteworthy that all veterans had previously completed prolonged exposure therapy for PTSD. Self-forgiveness and making amends are key intervention targets to restore spiritual well-being (9, 68). This is also the goal of Building Spiritual Strength, a group intervention for PTSD designed to be facilitated by either mental health providers or chaplains experienced in mental health counseling (69). Historically, chaplains have been major providers of care for military experience-related problems, including moral injury (70). Pastoral narrative disclosure is an intervention-based on a confessional model, developed specifically for use by chaplains (71). The focus of pastoral narrative disclosure is to have individuals reflect on the morally injurious experience, consider the guilt and shame, seek forgiveness, and reconnect with themselves and others. Direct participation from chaplains, clergy, and religious communities in the treatment process provides insight and support to help address the spiritual issues that arise from moral injury (18, 21). The value of incorporating chaplains into health care has been emphasized by both Departments of Defense and Veterans Health Administration (22, 72, 73).
As noted above, negative self-referential emotions such as guilt and shame are core symptoms of moral injury. Functional imaging studies in healthy individuals have begun to identify the areas activated by different self-referential emotions (5, 6). A systematic review summarized the neural correlates of guilt, embarrassment, and shame (5). Guilt was more likely associated with activity in the ventral anterior cingulate cortex, posterior temporal regions and the precuneus. Embarrassment was more likely to be associated with activity in the ventrolateral prefrontal cortex and amygdala. Shame was more likely to be associated with activity in the dorsolateral prefrontal cortex, posterior cingulate cortex, and sensorimotor cortex. Although guilt- and shame-activated distinct areas of the brain, there were also shared networks that involve emotional processing, self-referential processing, and social cognition (5). Although methodological approaches to guilt induction varied considerably, a recent meta-analysis of the neural correlates of guilt identified multiple areas, primarily in the left hemisphere (Figure 2) (6). Most relevant to understanding the neural correlates of emotional changes associated with development of moral injury (e.g., guilt, shame) are studies that utilized autobiographical scenarios to induce reexperiencing an emotional state (7, 8). Both studies reported activations in left precuneus/retrosplenial cortex and left inferior frontal gyrus/anterior insular cortex associated with negative (compared with neutral) self-referential scenarios (guilt, shame) (Figure 2) These areas were also activated by positive self-referential scenarios (pride) (7).

FIGURE 2. Negative self-referential emotions (guilt, shame) are core symptoms of moral injury. Functional imaging studies of healthy individuals have begun to identify the areas activated by different self-referential emotions (5, 6). A recent meta-analysis of the neural correlates of guilt identified multiple areas, primarily in the left hemisphere (red circles) (6). Most relevant to understanding the neural correlates of moral injury are studies that utilized autobiographical scenarios to facilitate reexperiencing a self-referential emotional state (7, 8). The reported cortical activations are color-coded by condition and study. Both studies reported activations in the left precuneus/retrosplenial cortex and left inferior frontal gyrus/anterior insular cortex associated with negative (compared with neutral) self-referential scenarios (guilt, shame). These areas were also activated by positive self-referential scenarios (pride) (7).
Although interventions designed to facilitate healing from moral injury are still in the early stages of development and testing, learning to forgive moral/ethical transgressions by self and others is a common theme (9–11). Studies have not yet addressed the neurobiology of forgiving serious transgressions by self or known others (74). Two studies of healthy individuals have identified neural correlates related to forgiving others for transgressions (Figure 3). A task-activated fMRI study reported higher activity in multiple areas (left dorsolateral prefrontal cortex, right inferior parietal lobule, bilateral middle temporal gyrus, posterior cingulate cortex, and occipital cortex) when participants were instructed to forgive compared with when they were instructed to not forgive offenders (12). A resting-state fMRI study reported that spontaneous activity (amplitude of low frequency fluctuation) in regions associated with mentalizing and self-referential processing (right dorsomedial prefrontal cortex, bilateral precuneus, left inferior parietal lobule) was negatively correlated with scores on the tendency to forgive scale (i.e., higher resting-state activity was associated with lower tendency to forgive transgressions by others) (13). In the absence of functional imaging studies on self-forgiveness, the neural correlates of loving kindness meditation may be informative. An fMRI study of experienced meditators reported that loving kindness meditation (compared with resting-state) resulted in both increases (left medial and anterior prefrontal cortices) and decreases (left parieto-occipital cortex) in activity (14). It is noteworthy that the areas of decreased activity partially overlap with areas in which lower resting-state activity correlated with higher forgiveness (13, 14).

FIGURE 3. A common theme of interventions to promote healing from moral injury is the importance of forgiveness (9–11). Two studies of healthy individuals have identified neural correlates related to forgiving others for transgressions (12, 13). The task-activated functional MRI (fMRI) study reported higher activity in multiple areas (pink) when participants were instructed to forgive compared with when they were instructed to not forgive offenders (12). The resting-state fMRI study reported that higher scores on the tendency to forgive scale (i.e., more likely to forgive transgressions by others) were negatively correlated with spontaneous activity (amplitude of low frequency fluctuation [ALFF]) in regions associated with mentalizing and self-referential processing (blue) (13). In the absence of studies on self-forgiveness, the neural correlates of loving kindness meditation may be informative. An fMRI study of experienced meditators reported that loving kindness meditation (compared with resting-state) was associated with both increases (orange) and decreases (green) in activity (14). Of note, the areas of decreased activity partially overlap with areas in which lower resting-state activity correlated with a higher tendency to forgive (13, 14).
In summary, although the research is early stage, there is growing evidence that the neurobiology underlying PTSD may differ by index trauma type. Moral injury, while often coexistent with PTSD, is not fear-based. Elucidating the neural correlates of moral injury, while extremely difficult in laboratory settings, would be valuable in guiding development of successful therapies. Challenges include the need to induce strong, predictable, and reproducible emotional states, incorporation of individually specific factors such as spiritual background, culture, community, and the nature of the trauma.
1 : Different neural modifications underpin PTSD after different traumatic events: an fMRI meta-analytic study. Brain Imaging Behav 2016; 10:226–237Crossref, Medline, Google Scholar
2 :
3 :
4 : Resting-state brain fluctuation and functional connectivity dissociate moral injury from posttraumatic stress disorder. Depress Anxiety (Epub ahead of print, January 28, 2019)Google Scholar
5 : Feelings of shame, embarrassment and guilt and their neural correlates: a systematic review. Neurosci Biobehav Rev 2016; 71:455–471Crossref, Medline, Google Scholar
6 : Neural mapping of guilt: a quantitative meta-analysis of functional imaging studies. Brain Imaging Behav 2017; 11:1164–1178Crossref, Medline, Google Scholar
7 : Brain activation associated with pride and shame. Neuropsychobiology 2014; 69:95–106Crossref, Medline, Google Scholar
8 : “Imagined guilt” vs “recollected guilt”: implications for fMRI. Soc Cogn Affect Neurosci 2016; 11:703–711Crossref, Medline, Google Scholar
9 : “Opening a door to a new life”: the role of forgiveness in healing from moral injury. Front Psychiatry 2018; 9:498Crossref, Medline, Google Scholar
10 : Is and ought: descriptive and prescriptive cognitions in military-related moral injury. J Trauma Stress 2019Crossref, Google Scholar
11 : Moral injury: an integrative review. J Trauma Stress(Epub ahead of print, January 28, 2019)Google Scholar
12 : How the brain heals emotional wounds: the functional neuroanatomy of forgiveness. Front Hum Neurosci 2013; 7:839Crossref, Medline, Google Scholar
13 : The neural association between tendency to forgive and spontaneous brain activity in healthy young adults. Front Hum Neurosci 2017; 11:561Crossref, Medline, Google Scholar
14 .: Structural changes in socio-affective networks: multi-modal MRI findings in long-term meditation practitioners. Neuropsychologia 2018; 116:26–33Crossref, Medline, Google Scholar
15 : An exploration of the viability and usefulness of the construct of moral injury in war veterans. Traumatology 2011; 17:8–13Crossref, Google Scholar
16 : Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin Psychol Rev 2009; 29:695–706Crossref, Medline, Google Scholar
17 : Moral injury in veterans of war. PTSD Res Quarterly 2012; 23:1–6Google Scholar
18 : Moral injury, soul repair, and creating a place for grace. J Relig Educ 2015; 110:382–394Crossref, Google Scholar
19 : Learning about combat stress from Homer’s Iliad. J Trauma Stress 1991; 4:561–579Crossref, Google Scholar
20 : Moral injury. Psychoanal Psychol 2014; 31:182–191Crossref, Google Scholar
21 : Moral injury and definitional clarity: betrayal, spirituality and the role of chaplains. J Relig Health 2017; 56:1212–1228Crossref, Medline, Google Scholar
22 : Moral injury: contextualized care. J Med Humanit 2018; 39:93–99Crossref, Medline, Google Scholar
23 : Defining and assessing moral injury: a syndrome perspective. Traumatology 2016; 22:122–130Crossref, Google Scholar
24 : Psychometric properties of a Modified Moral Injury Questionnaire in a military population. Traumatology2018; 24:301–312Crossref, Medline, Google Scholar
25 : Measuring symptoms of moral injury in veterans and active duty military with PTSD. 2018; 9:86Google Scholar
26 : Initial psychometric evaluation of the Moral Injury Questionnaire–Military version. Clin Psychol Psychother 2015; 22:54–63Crossref, Medline, Google Scholar
27 : Measuring moral injury: psychometric properties of the Moral Injury Events Scale in two military samples. Assessment 2016; 23:557–570Crossref, Medline, Google Scholar
28 : Sources of moral injury among war veterans: a qualitative evaluation. J Clin Psychol 2018; 74:2203–2218Crossref, Medline, Google Scholar
29 : Morally injurious experiences and meaning in Salvadorian teachers exposed to violence. Psychol Trauma 2015; 7:24–33Crossref, Medline, Google Scholar
30 : A scoping study of moral injury: Identifying directions for social work research. 2016; 70:190–200Google Scholar
31 : Journalists covering the refugee and migration crisis are affected by moral injury not PTSD. JRSM Open 2018; 9:2054270418759010Crossref, Google Scholar
32 : The emotional fallout from the culture of blame and shame. JAMA Pediatr 2017; 171:1141Crossref, Medline, Google Scholar
33 : The role of moral suffering (moral distress and moral injury) in police compassion fatigue and PTSD: an unexplored topic. Front Psychol 2017; 8:1999Crossref, Medline, Google Scholar
34 : Posttraumatic stress disorder in emergency medicine residents: a role for moral injury? Ann Emerg Med 2018; 72:322–323Crossref, Medline, Google Scholar
35 : Mechanisms of moral injury following military sexual trauma and combat in post-9/11 US war veterans. Front Psychiatry 2018; 9:520Crossref, Medline, Google Scholar
36 : The role of moral emotions in military trauma. Rev Gen Psychiatry. 2014; 18:249–262Crossref, Google Scholar
37 : A relative weights comparison of trauma-related shame and guilt as predictors of DSM-5 posttraumatic stress disorder symptom severity among US veterans and military members. Br J Clin Psychol 2018; 57:163–176Crossref, Medline, Google Scholar
38 : A critical outlook on combat-related PTSD: review and case reports of guilt and shame as drivers for moral injury. Mil Behav Health 2018; 6:156–164Crossref, Google Scholar
39 : Moral injury process and its psychological consequences among Israeli combat veterans. J Clin Psychol 2018; 74:1526–1544Crossref, Medline, Google Scholar
40 : Distinguishing war-related PTSD resulting from perpetration- and betrayal-based morally injurious events. Psychol Trauma 2017; 9:627–634Crossref, Medline, Google Scholar
41 : Indirect relations between transgressive acts and general combat exposure and moral injury. Mil Med 2017; 182:e1950–e1956Crossref, Medline, Google Scholar
42 : Negative outcomes after morally injurious experiences: a replication and extension. Psychol Trauma 2018; 10:456–462Crossref, Medline, Google Scholar
43 : Moral injury, meaning making, and mental health in returning veterans. J Clin Psychol 2015; 71:229–240Crossref, Medline, Google Scholar
44 : Perceptions of institutional betrayal predict suicidal self-directed violence among veterans exposed to military sexual trauma. J Clin Psychol 2016; 72:743–755Crossref, Medline, Google Scholar
45 : Moral injury, posttraumatic stress disorder, and suicidal behavior among National Guard personnel. Psychol Trauma 2018; 10:36–45Crossref, Medline, Google Scholar
46 : Morally injurious events and psychological distress among veterans: examining the mediating role of religious and spiritual struggles. Psychol Trauma 2018; 10:360–367Crossref, Medline, Google Scholar
47 : Roles of guilt cognitions in trauma-related sleep disturbance in military veterans with posttraumatic stress disorder. Behav Sleep Med doi: 10.1080/15402002.2018Google Scholar
48 : Latent profile analysis exploring potential moral injury and posttraumatic stress disorder among military veterans. J Clin Psychol 2019; 75:499–519Crossref, Medline, Google Scholar
49 :
50 : A network-based neurobiological model of PTSD: evidence from structural and functional neuroimaging studies. Curr Psychiatry Rep 2017; 19:81Crossref, Medline, Google Scholar
51 : Mindfulness-based treatments for posttraumatic stress disorder: a review of the treatment literature and neurobiological evidence. J Psychiatry Neurosci 2018; 43:7–25Crossref, Medline, Google Scholar
52 : Functional neuroanatomy of emotion and its regulation in PTSD. Harv Rev Psychiatry 2018; 26:116–128Crossref, Medline, Google Scholar
53 : Reductions in self-blame cognitions predict PTSD improvements with cognitive processing therapy for military sexual trauma-related PTSD. Psychiatry Res 2018; 263:181–184Crossref, Medline, Google Scholar
54 : Using prolonged exposure and cognitive processing therapy to treat veterans with moral injury-based PTSD: two case examples. Cognit Behav Pract 2018; 25:377–390Crossref, Medline, Google Scholar
55 : Adaptive disclosure: an open trial of a novel exposure-based intervention for service members with combat-related psychological stress injuries. Behav Ther 2012; 43:407–415Crossref, Medline, Google Scholar
56 : Loving-kindness in the treatment of traumatized refugees and minority groups: a typology of mindfulness and the nodal network model of affect and affect regulation. J Clin Psychol 2013; 69:817–828Crossref, Medline, Google Scholar
57 : Rationale for spiritually oriented cognitive processing therapy for moral injury in active duty military and veterans with posttraumatic stress disorder. J Nerv Ment Dis 2017; 205:147–153Medline, Google Scholar
58 : Spiritually integrated cognitive processing therapy: a new treatment for post-traumatic stress disorder that targets moral injury. Glob Adv Health Med 2018; 7:2164956118759939Crossref, Google Scholar
59 : Employing loving-kindness meditation to promote self- and other-compassion among war veterans with posttraumatic stress disorder. Spiritual Clin Pract 2018; 5:201–211Crossref, Google Scholar
60 : Loving-kindness meditation for posttraumatic stress disorder: a pilot study. J Trauma Stress 2013; 26:426–434Crossref, Medline, Google Scholar
61 : Mindfulness-based stress reduction for posttraumatic stress symptoms: building acceptance and decreasing shame. J Evid Based Complementary Altern Med 2014; 19:227–234Crossref, Medline, Google Scholar
62 : Loving-kindness meditation and the broaden-and-build theory of positive emotions among veterans with posttraumatic stress disorder. Med Care 2014; 52(Suppl 5):S32–S38Crossref, Medline, Google Scholar
63 : A pilot study of the effects of mindfulness-based stress reduction on post-traumatic stress disorder symptoms and brain response to traumatic reminders of combat in Operation Enduring Freedom/Operation Iraqi Freedom combat veterans with post-traumatic stress disorder. Front Psychiatry 2017; 8:157Medline, Google Scholar
64 : Spiritual interventions in veterans with PTSD: a systematic review. J Relig Health 2018; 57:2033–2048Crossref, Medline, Google Scholar
65 : Moral injury: a new challenge for complementary and alternative medicine. Complement Ther Med 2016; 24:29–33Crossref, Medline, Google Scholar
66 : “I knew it was wrong the moment I got the order”: a narrative thematic analysis of moral injury in combat veterans. Psychol Trauma 2018; doi: 10.1037/tra0000364 PubMedGoogle Scholar
67 .: A functional approach to understanding and treating military-related moral injury. J Context Behav Sci 2017; 6:391–397Crossref, Google Scholar
68 : Impact of killing in war: a randomized, controlled pilot trial. J Clin Psychol 2017; 73:997–1012Crossref, Medline, Google Scholar
69 : Spiritually integrated care for PTSD: a randomized controlled trial of “building spiritual strength”. Psychiatry Res 2018; 267:420–428Crossref, Medline, Google Scholar
70 : Moral injury, spiritual care and the role of chaplains: an exploratory scoping review of literature and resources. J Relig Health 2016; 55:1218–1245Crossref, Medline, Google Scholar
71 : Chaplaincy, spiritual care and moral injury: considerations regarding screening and treatment. Front Psychiatry 2018; 9:619Crossref, Medline, Google Scholar
72 : Implementing integrated mental health and chaplain care in a National Quality Improvement Initiative. Psychiatr Serv 2017; 68:1213–1215Crossref, Medline, Google Scholar
73 : Spiritual dimensions of moral injury: contributions of mental health chaplains in the Canadian Armed Forces. Front Psychiatry 2018; 9:592Crossref, Medline, Google Scholar
74 : The neural systems of forgiveness: an evolutionary psychological perspective. Front Psychol 2017; 8:737Crossref, Medline, Google Scholar