Drug-Responsive Mania in a Man With a Brain Tumor
SIR: We report a case in which a large temporal lobe tumor induced a classic presentation of manic psychosis that was rapidly responsive to neuroleptic treatment.
Case Report
A 61-year-old man was admitted for his first psychiatric hospitalization after a several-week history of severe, progressive changes in mood and behavior. At the time of admission, the patient exhibited decreased need for sleep, increased energy, racing thoughts, mood lability, hypersexuality, bizarre behavior, and grandiose delusions. His neurologic examination was nonfocal. His mental status examination was remarkable for mania and psychosis. There was no history of seizures.
The patient's past medical history was significant only for aqueductal stenosis. This was diagnosed incidentally by MRI following an episode of loss of consciousness 1 year prior to admission. This initial MRI demonstrated no mass lesions or midline shift. A 24-hour EEG and neurological examination were both normal at that time. A follow-up MRI 5 months prior to the current admission was again remarkable only for aqueductal stenosis, with no episodes of seizure or loss of consciousness reported by the patient. The patient had no prior psychiatric contact, but he reported mild mood swings for the past 10 years, consisting of periods during which he had more energy, needed less sleep, and worked 70 hours per week, followed by periods of lethargy, increased sleep, and blue mood.
During the current admission, the patient was treated for psychotic mania with perphenazine 28 mg bid. The bizarre behavior and delusions remitted within 1 week, and the remaining symptoms diminished within 2 weeks. A gadolinium-enhanced MRI was performed as a routine follow-up for the previous diagnosis of aqueductal stenosis. The results revealed a 5×3×4-cm mass in the right temporal lobe, with surrounding necrosis and hemorrhage, as shown in Figure 1. The patient was subsequently transferred to the Neurosurgery Service for surgical resection of the mass. The final pathology was consistent with glioblastoma multiforme. Perphenazine was discontinued postoperatively. The patient was discharged home on phenytoin and dexamethasone to a 7-week course of radiation therapy.
It is well known that symptoms referable to a brain tumor can vary based on the location of the mass. Although tumors of the temporal lobe can be associated with psychotic symptoms,1 this case is remarkable in that, despite the presence of a large, fast-growing right temporal lobe glioblastoma multiforme, the patient dramatically and rapidly responded to neuroleptic treatment. This finding suggests that the psychotogenic process caused by the tumor could be interrupted by a dopamine-blocking agent and supports clinical experience indicating that psychoses induced by known organic etiologies (e.g., drug-induced psychoses) may be reversed by neuroleptic treatment.
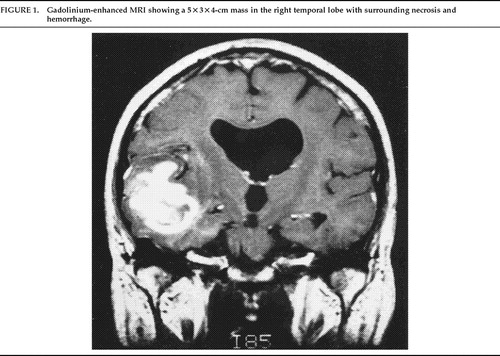
FIGURE 1. Gadolinium-enhanced MRI showing a 5×3×4-cm mass in the right temporal lobe with surrounding necrosis and hemorrhage.
1 Malamud N: Psychiatric disorder with intracranial tumors of the limbic system. Arch Neurol 1967; 17:113–123Crossref, Medline, Google Scholar