A Reality Test
Abstract
Psychosis in Parkinson’s disease (PD) is a major source of distress to patients and caregivers. Although the advent of atypical antipsychotic agents has, to some extent, resolved a clinical dilemma by preserving motor function while treating psychosis, our understanding of psychosis in PD remains in a nascent state. In this article the authors address several issues relating to psychosis in PD including the following: 1) prevalence, 2) possible etiologies and risk factors and 3) treatment. They also identify limitations in our understanding of this complex phenomenon and conclude that, despite availability of reasonable treatments for psychosis in PD, the search for a better understanding of the phenomenon must continue.
Psychosis in Parkinson’s disease (PD) is a risk factor for nursing home placement and, in association with dementia, increases morbidity and mortality.1,2 In addition to the cost and disability, psychosis may cause overwhelming caregiver burden.3 Prior to the advent of the atypical antipsychotic agents, attempts to treat psychotic symptoms led to inevitable worsening of motor function. Despite some encouraging advances in treatment strategies, our understanding of psychosis in PD remains in its infancy.
At this point, we still do not have a uniform definition of psychosis in PD or a universally accepted rating scale to gauge treatment response. In the PD literature, the term psychosis has been used to describe different behaviors by different authors. This lack of uniform classification is bound to generate controversy in the interpretation of study outcomes. There are some aspects of psychosis in PD that are universally accepted among those caring for patients with this illness. For example, unlike auditory hallucinations that are seen in primary psychiatric disorders (e.g. schizophrenia), the hallucinations in PD-associated psychosis are mainly visual. Other aspects of PD psychosis are subject to debate. For example, some would consider vivid dreams an early manifestation of psychosis whereas others would not.
In this article, we raise and begin to answer some fundamental questions regarding psychosis in PD. We conducted Medline searches using terms such as Parkinson’s disease and psychosis, then chose relevant articles from the references of our initial search. Subsequently, we reviewed literature related to some other conditions (e.g. DLB, sleep disorders) as their importance to the understanding of PD psychosis became evident. We review and integrate data obtained and theories proposed by others with our own experience. Based on this synthesis, we propose (where relevant) approaches to clinical care and future research. We focus on the following issues related to psychosis in PD: 1) prevalence, 2) possible etiologies and risk factors and 3) treatment.
WHAT IS THE PREVALENCE OF PSYCHOSIS IN PD?
Prevalence estimates of psychosis in PD have ranged from 3% for delusions4 to 30% for visual hallucinations.5–7 These rates are higher (5–62%) in studies that have included unselected parkinsonian patients with varied “psychotic phenomena” such as agitated confusion, reversible psychosis, and hallucinosis in addition to hallucinations and delusions.5,8,9
In prevalence studies, few authors have stratified their samples based on psychopathology, comorbid diagnoses, or types of medications. In a review of psychiatric side effects in 908 patients receiving levodopa, Goodwin found rates of 3.6% for both agitation and for psychosis.10 Another review reported that the prevalence of visual hallucinations (in the context of a clear sensorium) in PD patients receiving chronic antiparkinsonian therapy ranged from 9–32%.11 A recent prospective study evaluated prevalence of visual hallucinations in patients with PD. In this study of 98 patients, 26 had visual hallucinations. Among these, one patient also had delusions and two had auditory hallucinations.12 Another study6 attempted to stratify patients based on severity of psychosis using the Unified Parkinson’s Disease Rating Scale (UPDRS).13 Among 235 patients from the community, 24% of patients had vivid dreams believed to represent early stages of perceptual and thought disturbance, 10% had hallucinations with retained insight, and 6% had severe, persistent hallucinations without insight and/or delusions. The authors had excluded patients with previous histories of psychosis, but not those with dementia or depression.
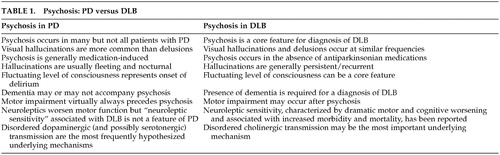
A study14 of 172 consecutive patients with 5-year histories of PD demonstrated a psychosis prevalence rate of 27%. In this case, the authors specifically excluded patients who developed dementia within one year of motor impairment and those in whom dementia predated the onset of motor symptoms, thereby making the inclusion of patients who had Dementia with Lewy bodies (DLB) less likely. This is important since the clinical similarities between patients who have PD complicated by dementia and psychosis and those with DLB can sometimes make diagnosis difficult. Various criteria have been proposed for DLB, in response to ongoing controversies.15,16 In practice, DLB is part of the differential diagnosis of Alzheimer's disease (AD) when the initial symptoms are cognitive and of PD when the initial symptoms are motor. Based on our review of the literature and our own experiences we have summarized some distinctions between psychosis in PD and DLB in Table 1.17,18
In summary, it is difficult to establish precise prevalence rates for “psychosis” in PD, given the varying interpretations of this term among investigators conducting studies thus far. Suffice it to say that studies to date support the notion that hallucinations are significantly more common than delusions and that psychotic phenomenon occur in at least 20% of medication-treated PD patients. Developing and implementing uniform diagnostic criteria (that are careful to exclude patients with DLB as best we can) will help us achieve a more accurate estimate of prevalence.
WHAT ARE THE POSSIBLE ETIOLOGIES AND RISK FACTORS FOR PSYCHOSIS IN PD?
The etiological basis of psychosis in PD remains an unsettled issue. Although there is some controversial evidence that psychosis was observed in PD patients before the advent of levodopa therapy,19,20 it is generally accepted that psychosis in PD is a drug-induced phenomenon. Many clinicians and researchers (including ourselves) believe that diagnoses other than idiopathic PD (e.g. DLB) should be considered in patients who develop psychosis early in the treatment with medications or those who develop psychosis without the use of implicated medications.21,22
However, the precise relationship between dopaminergic medications and psychosis has not been clearly delineated. The dose and duration of dopaminergic therapy are not considered consistent risk factors for hallucinations. Goetz et al.23 studied PD patients with a history of chronic hallucinations, noting that intravenous infusions of high-dose levodopa did not precipitate hallucinations. These observations suggest that the dopaminergic system is involved in the pathophysiologic process of hallucinations in PD, but that hallucinations themselves are not directly related to plasma (and presumably brain) levodopa levels.
The mechanisms that underlie PD psychosis remain to be determined. The most frequently proposed hypothesis is that, in some patients, denervation hypersensitivity of mesolimbic and mesocortical dopamine receptors may occur and that dopaminergic medications may stimulate these receptors to cause psychosis.9,24
More recently, it has been hypothesized that a combination or combinations of neurotransmitter systems play a role in the development of PD psychosis. Birkmayer and Riederer25 have suggested that a serotonergic/dopaminergic imbalance may be most important. In support of this notion are postmortem studies revealing variable degrees and distributions of serotonin loss among patients with PD26 and reports that pharmacological agents that exert their effects on serotonin receptors (e.g., atypical antipsychotics, ondansetron) appear to have some efficacy against PD-related visual hallucinations.27,28
Although deficiencies in cholinergic transmission are linked more closely to AD, there has been some suggestion that the ratio of serotonin to acetylcholine may be important for the development of psychosis in DLB.29,30 Profound depletion of cholinergic markers and relative preservation of serotonergic markers in the temporal or parietal cortex have been suggested as a possible neurochemical explanation for psychosis in DLB.29 This would be in keeping with the finding that acetylcholinesterase inhibitors might have some antipsychotic efficacy in these illnesses. Whether or not this is relevant to patients with PD and drug-induced psychosis remains to be determined.
An important question is why, when exposed to the same dopaminergic medications, do some PD patients develop psychosis while others do not? Based on established links in AD between psychosis and dopamine receptor genetic variants and APOE alleles, Goetz et al31 conducted a case-control study in PD patients with and without visual hallucinations. They determined, however, that visual hallucinations in PD are not associated with the genetic pattern seen for patients with AD and psychosis. The authors noted that comparison of serotonergic receptor polymorphisms in cases and controls remains an area for future research.
Whether or not specific antiparkinsonian agents are associated with different degrees or forms of psychosis is not clear. Some have reported that patients being treated with anticholinergics are likely to present with confusion and that hallucinations in these cases are less formed than with dopaminergic-induced psychosis.5,32 A recent 5-year study comparing the incidence of dyskinesia in PD patients treated with the dopamine agonist ropinirole or levodopa33 revealed that the incidence of hallucinations was higher in the ropinirole group (17% versus 6%). Similarly, dopamine agonist bromocriptine treatment was associated with more hallucinations34 in an open-label randomized trial comparing bromocriptine with the catechol-o-methyl-transferase (COMT) inhibitor tolcapone. In a smaller study involving 40 PD patients35 a switch from tolcapone as an adjunctive therapy to another COMT-inhibitor (entacapone) failed in 6 patients due to increase in dyskinesia and hallucinations.
Thus, it appears that while all antiparkinsonian medications may play a role in PD psychosis, some classes of medications (e.g., dopamine agonists) may do so more often. Additionally, clinicians need to consider the fact that many patients use other offending agents to control associated conditions (e.g., anticholinergic agents for bladder dysfunction).
Proposed risk factors for the development of psychosis in PD have included age, stage and severity of PD, depression, sleep disturbances, and cognitive impairment.6,12,14
Among the proposed risk factor for psychosis in PD, dementia emerges in the majority of studies.6,7,36 The precise relationship between dementia and psychosis is not clear. Does cognitive impairment contribute to symptoms of psychosis? (e.g., Do memory disturbances lead demented patients to believe that someone must have “stolen” from them?). Do dementia and psychosis stem from similar neuropathological and pathophysiological disease states, rendering the same patients vulnerable to both? (e.g. combined deficiencies of dopamine and acetylcholine, extension of Lewy body pathology beyond the brainstem).
Studies exploring the relationship between cognition and psychosis in similar neurodegenerative disorders (e.g. DLB) may help us understand the relationship between cognitive impairment and psychosis in PD.29,37 In a recent study37 neuropsychiatric symptoms were assessed in PD patients with dementia (PDD), PD patients without dementia (PDND) and in those with DLB (confirmed by autopsy in one-third). Delusions and hallucinations occurred with increasing frequency in PDND (7% and 14%), PDD (29% and 54%), and DLB (57% and 76%). The types of hallucinations and delusions were similar across the three groups. The authors commented that these findings add support to the hypothesis that psychiatric symptoms may be associated with cortical Lewy bodies or cholinergic deficits in both PD and DLB.
Our ability to understand the relationship between psychosis and dementia in patients with PD is further complicated by the relationship between dementia and delirium. Advanced age, pre-existing dementia and “organic brain disease” are all risk factors for delirium38,39 with up to 40% of delirious patients having dementia.40 It has been estimated that hallucinations occur in 30–77% of patients with delirium.41 We suggest that psychosis occurring in demented PD patients during delirium (“confusional psychosis”) may be different (both in pathophysiology and approach to treatment) than psychosis occurring in cognitively intact PD patients in the setting of a clear sensorium.
There appears to be a strong relationship between sleep disturbances and psychosis in PD. Whether sleep disturbances are a risk factor for psychosis in PD or if sleep disturbances represent one end of the “psychosis spectrum” in PD continues to be debated.
Moskovitz et al.9 applied the model of pharmacological kindling in an attempt to understand progressively abnormal behavioral alterations in patients receiving levodopa therapy for PD. In their sample of 88 PD patients, all psychotic states were associated with preexistent or concurrent vivid dreams and/or hallucinations. In another study,42 the majority of patients who had psychiatric side effects from levodopa also had sleep disturbances in the form of excessive daytime sleepiness, parasomnias (e.g., sleep walking, sleep talking) and nocturnal myoclonus. Among patients with sleep alteration, 39% were hallucinating compared to only 4% who did not have sleep disruption.
Although many forms of sleep disturbances are described in PD, rapid-eye movement (REM)-related sleep disorders appear most closely related to psychosis. Altered dream activity in PD patients can include vivid dreams, nightmares and other REM behavior disorders, such as nocturnal vocalization and movements.43 Several lines of evidence suggest a fundamental link between the processes underlying REM sleep disturbances and those responsible for psychosis in PD. Reduced REM sleep is observed more often in patients who hallucinate than in those who do not.44 Some have suggested that psychosis in PD may reflect a narcolepsy-like REM sleep disorder.45 In one study, polysomnographic (PSG) recordings were obtained on 20 patients with PD (half experienced levodopa-induced hallucinations and half did not). The patients with a history of hallucinations had narcolepsy-like REM sleep episodes that coincided with hallucinations during the day and post-REM delusions at night.
In summary, psychosis in PD appears to be a drug-induced phenomenon. Antiparkinsonian medications alone, however, are not sufficient to cause psychosis (given the fact that only some medicated PD patients develop psychosis). There are likely to be neuropathological and pathophysiological differences among patients that result in the development of psychosis in some but not others. Supersensivity of mesolimbic and mesocortical dopaminergic systems are likely to be involved but nondopaminergic systems (and serotonin in particular) are probably important as well. Further elucidation of the close relationships between psychosis and what are currently viewed as its biggest risk factors (dementia and sleep disorders) may provide insights into underlying mechanisms.
HOW DO WE TREAT PSYCHOSIS IN PD?
Confirmation of Diagnosis
The first step in management is to ensure that the altered behavior truly represents psychosis. Disorders of vision may cause illusions that are recorded as hallucinations. Cognitively impaired patients may misplace objects and assert that caretakers have stolen them.
A list of all current medications, including any recent additions, deletions or dosage changes should be reviewed. If the patient appears to have a clouded consciousness with fluctuating levels of alertness, delirium should be suspected. Delirium may occur in a patient who has dementia with PD, or a PD patient who has a superimposed medical condition such as pneumonia or a urinary tract infection. Older patients in advanced stages of PD who have cognitive deficits and are taking several medications are at the highest risk. Diagnostic consideration of DLB should also be considered since fluctuating levels of consciousness and cognition are characteristic symptoms of this illness.
Psychosocial Strategies
It is well established that elderly patients with psychosis require a higher level of support. The clinician needs to assess the nature and degree of psychosis, as well as its functional and social impact on the patient, caregiver and family members. Caregivers need to understand what psychosis is, what they can and cannot do to help, and where they can get support. Regulating the environment may help prevent escalation of psychotic symptoms. Increased light during the day and decreased light at night may improve orientation and minimize excessive sensory stimulation. Psychosis (particularly in cognitively impaired patients) is frequently associated with agitation. Agitated patients should be approached in a calm manner. Instead of confronting the patient or making demands, it may prove helpful to use distractions and communicate the desire to help. Agitated patients can sometimes become aggressive. Safety of the patient and those around him or her is paramount. The development of aggressive, violent behavior may necessitate an urgent evaluation and possible psychopharmacological intervention (see below). Families may need support in their decisions regarding available treatments, hospitalizations, and plans for long-term placement. Consultation with psychiatric colleagues may be productive in terms of achieving optimal behavioral, psychological, and pharmacological interventions.
Pharmacological Strategies
1. Overview
Traditionally, clinicians attempted to reduce the dosages of antiparkinsonian agents and, only if unsuccessful, employed an antipsychotic agent. With the availability of atypical antipsychotic agents, some experts have started questioning the practice of dopaminergic dose reduction given the risk of motor deterioration and persistence of psychosis.46
Conventional or typical antipsychotics (i.e., neuroleptics) are not considered standard care in an era where atypical agents, theoretically less apt to worsen parkinsonian motor function, are available. The only atypical antipsychotic agent that has been tested in a large-scale, placebo-controlled clinical trial involving psychotic PD patients is clozapine.47 It was shown to be effective and well tolerated at low dosages. Unfortunately, clozapine has a potential risk for agranulocytosis, necessitating frequent blood monitoring. This makes it somewhat difficult and expensive to use. Other “atypical” antipsychotic agents (e.g., quetiapine) may offer similar efficacy and tolerability without the risk for agranulocytosis. However, as of yet, none have been subjected to rigorous testing in a large-scale, well-designed clinical trial. In addition to the atypical antipsychotics, medications with other mechanisms of action have been considered. These include agents that have primary effects on the neurotransmission of serotonin (e.g., ondansetron) and acetylcholine (e.g., acetyl cholinesterase inhibitors).
Just as there is no uniformly accepted definition of psychosis in PD, neither is there a uniformly accepted rating scale to measure the treatment response of antipsychotic agents in this illness. Most investigators have used existing psychosis ratings scales and, in some cases, modified them for use in PD. The Parkinsonian Psychosis Rating Scale (PPRS) was developed specifically for use in PD and was used in a 6-week open-label study evaluating ondansetron for the treatment of psychosis in 29 parkinsonian patients.48 This scale includes six dimensions that are commonly associated with psychosis in PD (visual hallucinations, illusions and misidentification, paranoid ideation, sleep disturbance, confusion, and sexual preoccupation). In addition to measuring the severity of symptoms, the scale contains a section for family and caregivers to report their impression of the patient's Global Functional Impairment (GFI).
Statistically significant reductions in mean scores for the six PPRS items were reported after 6-weeks of ondansetron treatment (see below). The authors concluded that the PPRS appears to be a specific measure of psychosis in PD and that paranoid ideation, hallucinations, and confusion appeared to have the greatest impact on patient and families.
2. Clozapine
Clozapine has greater affinity for D4 receptors than for D1 and D2 receptors. Its preferential ability to bind to mesolimbic rather than nigrostriatal neuronal receptors is believed to result in a significantly lower incidence of extrapyramidal syndromes (EPS) and makes it less apt to worsen motor features of PD.
An initial double-blind, placebo-controlled clinical trial of clozapine in PD patients with psychosis was discontinued after three of six patients who had been enrolled withdrew from the study.49 This study used a starting dose of 25 mg/day and daily increases by the same amount. Too high of an initial dose and rapid titration may have caused problems with tolerability.
More recently, the Parkinson Study Group completed a double-blind, placebo-controlled, multicenter clinical trial of low-dose clozapine for the treatment of drug-induced psychosis in PD.47 This study, involving 60 subjects, revealed that low dosages of clozapine were effective in reducing psychotic symptoms without worsening motor function. Clozapine was started at 6.25 mg and increased as needed up to 50 mg q.h.s. Patients in the clozapine group (mean dosage = 27 mg) showed significant improvement on all three measures of psychosis that were used including the Brief Psychiatric Rating Scale (BPRS),50 Scale for the Assessment of Positive Symptoms (SAPS)51 and the Clinical Global Impression (CGI) scale.52 There was no worsening of motor function (as measured by the UPDRS) and tremor improved. Fifty-three subjects completed an open-label extension for 12 weeks following completion of the four-week double-blind phase. The group that was switched from placebo to clozapine showed improvement, and both groups maintained the response throughout the duration of the open-label extension.53 The main disadvantage of clozapine therapy is the risk of agranulocytosis in 1–2% cases, which requires regular blood monitoring for all patients on this agent.
3. Risperidone
Risperidone has dosage dependent D2 antagonism in addition to its 5HT2 antagonism, anti-adrenergic and anti-histaminergic effects. It has limited effect on D1 and muscarinic receptors. The role of risperidone in the treatment of PD patients with psychosis is still being debated in the literature. Some open-label and retrospective studies suggested that psychosis in PD can be successfully treated with risperidone,55–58 but other reports have contrasting results.59,60 A double-blind comparison of clozapine and risperidone in nine patients demonstrated mental improvement in both groups and statistically nonsignificant worsening of motor symptoms in risperidone group.56 The authors noted that risperidone may be considered as an alternative to clozapine but indicated that it may worsen extrapyramidal symptoms more than clozapine and should be used with caution.
4. Olanzapine
Like clozapine, olanzapine has high affinity for M1 muscarinic, H1 histamine, D1 dopamine, and alpha1 adrenergic receptors with somewhat weaker D2 dopamine antagonism. Some open-label studies suggested that olanzapine resulted in a marked benefit in psychosis without a decline in motor function for PD patients.61,62 Later reports, however, were less glowing, and concerns arose regarding the use of olanzapine in PD. In one study involving 19 patients with atypical parkinsonian syndromes, almost half showed poor tolerability of olanzapine.63 Motor features improved in three patients but worsened in 10. One patient required hospitalization due to marked worsening of parkinsonism. In another study, psychiatrically stable PD patients were switched from clozapine to olanzapine. Seventy-five percent of patients switched back to clozapine due to poor tolerability of olanzapine.64 A randomized double-blind parallel comparison of olanzapine and clozapine in PD patients with chronic hallucinations was discontinued because of worsened parkinsonism in olanzapine-treated subjects. The authors concluded that, in comparison with clozapine, olanzapine aggravates parkinsonism and should not be regularly used in management of hallucinations in patients with PD.65 Olanzapine also increased parkinsonism and “off” time in another small controlled double-blind crossover trial in which patients with PD received 2 weeks of olanzapine or placebo with a 1-week washout between phases.66
5. Quetiapine
Quetiapine's 5HT2A antagonism is more pronounced than its D2 antagonism. In addition, it has high affinity for alpha-1 adrenergic and histamine H1 receptors, lower affinity for D1 dopamine receptors and no muscarinic M1 activity.67 Quetiapine has received favorable verdicts in the literature regarding its use in psychosis associated with PD. It has not, however, been subjected to a double-blind, placebo-controlled clinical trial. Similar to clozapine, it does not antagonize apomorphine-induced stereotypy and is weakly cataleptic. Several studies in the elderly have found it safe, with sedation, dizziness, and hypotension being the most frequent side effects. Lenticular changes were noted during preclinical animal studies, leading the manufacturer to recommend periodic ophthalmologic examinations.68 Friedman et al reviewed seven studies involving a total of 123 patients with parkinsonism and psychosis. This heterogeneous group of patients included those with and without dementia and those with atypical parkinsonian syndromes. One hundred five patients were considered improved with regard to their psychosis, although 16 had worsening of motor symptoms.69 The same group reported their own experience with 69 PD patients, noting that 18% had a mild to moderate increase in their parkinsonism with quetiapine.70 Dewey et al conducted a retrospective review of their experience with quetiapine to assess its effectiveness and tolerability in PD patients with drug-induced psychosis. Sixty-one patients were available for adequate follow up, and 66% of them remained on quetiapine with good control of hallucinations. Nine patients had to be switched to clozapine due to inadequate response, and six stopped taking the drug for other reasons.71 In one recent abstract presentation72 quetiapine was reported to be effective in improving psychotic symptoms in patients with PD, without deterioration in the motor symptoms. Significant improvement in memory was observed in psychotic PD patients following 24 weeks of quetiapine therapy, suggesting that a subset of patients with PD and psychosis may experience improvement in immediate and delayed memory with quetiapine. In a small 3-month open-label trial of quetiapine in neuroleptic naïve patients with PD and psychosis, the mean dosage after 14 days was 138.6 mg/day, (maximum 225 mg/day). Data were available for 7 of 11 patients; all tolerated relatively high doses and none of them showed motor worsening.73 Reddy et al74 performed a retrospective record review of open-label quetiapine treatment for drug-induced psychosis in their PD patients. They concluded that quetiapine appears to be effective in improving psychosis in approximately 80% of PD patients, both with and without dementia. They noted, however, that patients with dementia seem to have a higher propensity for worsening motor symptoms. Sommer75 reported two cases of quetiapine-induced extrapyramidal side effects but noted that the patients were “unusual in their frailty and severity of illness and may not represent the majority of patients with PD.”
6. Other potential pharmacological agents:
Several other medications have been used to treat psychosis in PD, with mixed results. As noted above, ondansetron (a 5HT3 antagonist) showed partial or complete improvement in open-label studies of PD patients with psychosis.28,48 However, another trial failed to replicate these findings.76 Ziprasidone has recently been approved for the treatment of schizophrenia. It is an atypical antipsychotic, although it has a greater propensity to prolong the QT/QTc interval compared to other antipsychotics (package insert). At present, it is too early to determine whether or not this agent will have a role in the treatment of PD psychosis.
Acetylcholinesterase (AChE) inhibitors have been increasingly viewed as having the potential to improve behavior77 in addition to their accepted role as cognitive enhancers. Initial reports have been interesting.78–80 A case series of DLB patients demonstrated cognitive, functional, and behavioral improvements with the AChE inhibitor donepezil.79 However, it was also noted that one-third of the patients treated with donepezil had worsening of parkinsonism that responded to carbidopa/levodopa. In a double-blind, placebo-controlled trial of the AChE inhibitor rivastigmine in patients with DLB,80 120 patients received up to 12 mg of rivastigmine per day or placebo for 20 weeks. Patients taking rivastigmine had fewer delusions and hallucinations and greater cognitive improvement than controls. Analysis of UPDRS motor subscale revealed no change in parkinsonian symptoms on rivastigmine compared to baseline and placebo. A recent case report observed that pharmacologic challenge of a PD patient with one 3 mg dose of rivastigmine appeared to worsen motor and mood symptoms.81 The efficacy and tolerability of AChE inhibitors in PD patients with psychosis remains to be determined.
Electroconvulsive Therapy (ECT)
Electroconvulsive therapy is another modality occasionally used to treat PD patients with psychosis, especially those who are unable to tolerate medications such as clozapine. Improvements in motor symptoms have also been noted. It has been suggested that ECT may help psychiatric and motor states via dopaminergic and nondopaminergic mechanisms. The use of ECT followed by maintenance with low-dosage clozapine has been reported to be effective and well tolerated in PD and drug induced psychosis.82 There have, however, been no controlled trials of ECT in patients with PD and psychosis. The cognitive risks in older individuals have included disorientation, delirium, and amnesia. In a prospective study of seven consecutive patients with PD, there was 100% incidence of interictal delirium during the course of ECT.83 Patients with basal ganglia disease may be particularly vulnerable to ECT-induced delirium.84 Age and pre-ECT modified MMSE scores were found to be predictors of lower autobiographical recall.85 The available data support the conventional wisdom that preexisting cognitive impairment is a risk factor for the development of delirium and for a more severe ECT-induced amnesia.
In summary, it is important to have a high index of suspicion for drug-induced psychosis, particularly in PD patients with dementia. It is reasonable to review medication lists and remove any unnecessary psychotropic agents. However, it is no longer necessary to reduce the antiparkinsonian medications to the point of sacrificing mobility. There are several “atypical” antipsychotic agents currently available. The only one that has been subjected to the rigors of a large-scale clinical trial is clozapine. This agent was shown to be an effective antipsychotic agent in PD that does not impair mobility. However, from a practical standpoint, there are complexities (blood monitoring, regulation of drug dispensing) associated with its use and in practice it is frequently reserved for patients in whom another atypical antipsychotic proved ineffective or poorly tolerated. We believe that a large-scale clinical trial in which an atypical antipsychotic agent (e.g., quetiapine) is directly compared to clozapine would facilitate the practice of evidence-based medicine for this condition. In the meantime (regardless of the agent chosen), we suggest using very low initial dosages and monitoring motor function closely.
CONCLUSION
Psychosis in PD affects at least 20% of medicated patients and appears to be due to an interaction between PD-related pathophysiology and dopaminergic medications. Visual hallucinations are the most frequent form of psychosis in PD but delusions are not uncommon. Psychosis can occur in the setting of a clear or clouded sensorium. Classification of psychotic behavior is difficult within the constructs currently available. Further research to define diagnostic criteria for psychosis and its course and treatment outcomes in PD is needed.
The frequent coexistence of parkinsonism, dementia, and psychosis can make diagnosis difficult, and it is important to consider DLB in the differential diagnosis. The relative time of onset of motor and cognitive features may help with diagnosis. The nature of the psychosis and whether or not it was provoked by antiparkinsonian medications may also provide clues. However, it should be noted that the lines dividing these neurodegenerative conditions can prove indistinct, both from the clinical and pathological perspectives.
It has been hypothesized that, in some patients, denervation hypersensitivity of mesolimbic dopamine receptors may occur and that dopaminergic medications may stimulate these hypersensitive receptors to cause psychosis. The exact neurochemical link to the dopaminergic system, however, is not clearly delineated and the interplay among several neurotransmitters (including serotonin and acetylcholine) may be important. Proposed risk factors for the development of psychosis in PD have included age, stage and severity of PD, depression, sleep disturbances, and cognitive impairment,8,14,16 with the last two emerging as the strongest ones.
The availability of atypical antipsychotic medications such as clozapine, that can reduce psychosis while preserving motor function, have launched us into a new era of treatment for psychosis in PD. We await the results of well-controlled clinical trials involving other potential antipsychotic agents. The fact that effective treatments for psychosis in PD are now becoming a “reality” may “test” our resolve to genuinely understand this complex phenomenon. Further exploration of psychosis in PD may enable us to develop more focused approaches to its treatment and perhaps its prevention. In addition, by furthering our understanding of PD psychosis, we will undoubtedly learn more about other aspects of PD (e.g., dementia), related neurodegenerative diseases, (e.g. DLB) and primary psychotic disorders (e.g., schizophrenia).
 |
1 Goetz CG, Stebbins GT: Risk factors for nursing home placement in advanced Parkinson’s disease. Neurology 1993; 43:2227–2229Crossref, Medline, Google Scholar
2 Goetz CG, Stebbins GT: Mortality and hallucinations in nursing home patients with advanced Parkinson’s disease. Neurology 1995; 45:669–671Crossref, Medline, Google Scholar
3 Carter JH, Stewart BJ, Archold PG, et al: Living with persons who have Parkinson’s disease: The spouses' perspective by stage of the disease. Mov Disord 1998; 33:20–28Crossref, Google Scholar
4 Klawans HL: Levodopa-induced psychosis. Psychiatric An 1978; 8:447–451Google Scholar
5 Cummings JL: Neuropsychiatric complications of drug treatment of Parkinson’s disease, in Parkinson’s disease: Neurobehavioral aspects, edited by Huber SJ, Cummings JL. NY, Oxford University Press, 1992, pp 313–327Google Scholar
6 Aarsland D, Larsen JP, Cummings JL, et al: Prevalence and clinical correlates of psychotic symptoms in Parkinson’s disease. Arch Neurol 1999; 56:595–601Crossref, Medline, Google Scholar
7 Sanchez-Ramos JR, Ortoll R, Paulson GW: Visual hallucinations associated with Parkinson Disease. Arch Neurol 1996; 53:1265–1268Crossref, Medline, Google Scholar
8 Fischer P, Danielcyzk W, Simanyl M, et al: Dopaminergic psychosis in advanced Parkinson’s disease. Adv Neurol 1990; 53:391–397Medline, Google Scholar
9 Moskowitz C, Moses H, Klawans HL: Levodopa induced psychosis: a kindling phenomenon. Am J Psychiatry 1978; 1135:669–675Google Scholar
10 Goodwin FK: Psychiatric side effects of Levodopa in man. JAMA 1971; 218(13):1915–1920Crossref, Medline, Google Scholar
11 Goetz CG: Hallucinations in Parkinson’s disease: The clinical syndrome. Adv Neurol 1999; 80:419–423Medline, Google Scholar
12 Holroyd S, Currie L, Wooten GF: Prospective study of hallucinations and delusions in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2001; 70:734–738Crossref, Medline, Google Scholar
13 Fahn S, Elton RC and Members of UPDRS Development Committee: Unified Parkinson’s disease rating scale, in Recent developments in Parkinson’s disease, vol II, edited by Fahn S, Marsden DC, Goldstein M, et al. Florheim Park, NJ, Macmillan, 1997, pp 153–163Google Scholar
14 Giladi N, Treves TA, Paleacu D: Risk factors for dementia, depression and psychosis in long-standing Parkinson’s disease. J Neural Trans 2000; 107:59–71Crossref, Medline, Google Scholar
15 McKeith IG, Perry RH, Fairbairn AF et al: Operational criteria for senile dementia of Lewy body type (SDLT). Psychol Med 1992; 22:911–922Crossref, Medline, Google Scholar
16 Byrne EK, Lennox GG, Godwin-Austen RB, et al: Dementia associated with cortical Lewy bodies: proposed clinical diagnostic criteria. Dementia 1991; 2:283–284Google Scholar
17 Ballard C, Holmes C, McKeith I, et al: Psychiatric morbidity in dementia with Lewy bodies: a prospective clinical and neuropathological comparative study with Alzheimer's disease. Am J Psychiatry 1999; 156:1039–1045Medline, Google Scholar
18 Klatka LA, Louis ED, Schiffer RB: Psychiatric features in diffuse Lewy body disease: a clinicopathologic study using Alzheimer's disease and Parkinson’s disease comparison groups. Neurology 1996; 47:1148–1152Crossref, Medline, Google Scholar
19 Jackson JA, Free GBM, Pike HV: The psychic manifestation of paralysis agitans. Arch Neurol Psychiatry 1923; 10:680–684Crossref, Google Scholar
20 Schwab RS, Fabing HD, Prichard JS: Psychiatric symptoms and syndromes in Parkinson’s disease. Am J Psychiatry 1950; 107:901–907Crossref, Google Scholar
21 Litvan I, MacIntyre A, Goetz CG, et al: Accuracy of the clinical diagnosis of Lewy body disease, Parkinson’s disease and dementia with Lewy bodies: a clinicopathological study. Neurology 1998; 55:969–978Google Scholar
22 Goetz CG, Vogel C, Tanner CM, et al: Early dopaminergic drug-induced hallucinations in Parkinsonian patients. Neurology 1998; 51:811–814Crossref, Medline, Google Scholar
23 Goetz CG, Pappert EJ, Blasucci LM, et al: Intravenous Levodopa in hallucinating Parkinson’s disease patients: High dose challenge does not precipitate hallucinations. Neurology 1998; 50:515–517Crossref, Medline, Google Scholar
24 Wolters EC. Dopaminomimetic psychosis in Parkinson’s disease patients. Diagnosis and treatment. Neurol 1999; 52(3):10–13Crossref, Medline, Google Scholar
25 Birkmayer W, Riederer P. Responsibility of extrastriatal areas for the appearance of psychotic symptoms. J Neural Transm 1975; 37:175–182Crossref, Medline, Google Scholar
26 Jellinger K. The pathology of parkinsonism, in Movement Disorders, vol 2, edited by Marsden CD, Fahn S (International Medical Reviews, Neurology; vol 7), London, Butterworth, 1987, pp 124–165Google Scholar
27 Melamed E, Zoldan J, Freidberg G: Is hallucinosis in Parkinson’s disease due to central serotonergic hyperactivity? Mov Disord 1993; 8:406–407Google Scholar
28 Zoldan J, Friedberg G, Goldberg-Stern H, et al: Ondansetron for hallucinosis in advanced Parkinson’s disease. Lancet 1993; 341:562–563Crossref, Medline, Google Scholar
29 Perry EK, Marshall E, Kerwin JM, et al: Evidence of a monoaminergic: cholinergic imbalance related to visual hallucinations in Lewy body dementia. J Neurochem 1990; 55:1454–1456Crossref, Medline, Google Scholar
30 Perry EK, McKeith I, Thompson P, et al: Topography, extent, and clinical relevance of neurochemical deficits in dementia of Lewy body type, Parkinson’s disease, and Alzheimer's disease. Ann NY Acad Sci 1991; 640:197–202Crossref, Medline, Google Scholar
31 Goetz CG, Burke PF, Leurgans S, et al. Genetic variation analysis in Parkinson Disease patients with and without hallucinations: Case-control study. Arch Neurol 2001, 58:209–213Google Scholar
32 Cummings JL: Behavioral complications of drug treatment of Parkinson’s disease. J Am Geriatr Soc 1991; 39:708–716Crossref, Medline, Google Scholar
33 Rascol O, Brooks DJ, Korczyn AD, et al: A five year study of the incidence of dyskinesia in patients with early Parkinson’s disease who were treated with Ropinirole or Levodopa. NEJM 2000; 342(20):1484–1491Crossref, Medline, Google Scholar
34 Tolcapone Study Group: Efficacy and tolerability of tolcapone compared with Bromocriptine in Levodopa-treated Parkinsonian patients. Mov Disord 1999; 14(1):38–44Crossref, Medline, Google Scholar
35 Onofrj M, Thomas A, Iacono D, et al: Switch-over from tolcapone to entacapone in severe Parkinson’s disease patients. Eur Neurol 2001; 46(1):11–6Crossref, Medline, Google Scholar
36 Naimark D, Jackson E, Rockwell E, et al: Psychotic symptoms in Parkinson’s disease patients with dementia. J Am Geriatric Soc 1996; 44:296–299Crossref, Medline, Google Scholar
37 Aarsland D, Ballard C, Larsen JP, et al: A comparative study of psychiatric symptoms in dementia with Lewy bodies and Parkinson’s disease with and without dementia. Int J Geriatr Psychiatry 2001; 16:528–536Crossref, Medline, Google Scholar
38 Koponen HJ, Rickkinen PJ: A retrospective study of delirium in elderly patients admitted to a psychiatric hospital. Psychol Med 1993; 23:103–109Crossref, Medline, Google Scholar
39 Sandberg G, Gustafsen Y, Brannstrom B, et al: Clinical profile of delirium in older patients. J Am Geriatr Soc 1999; 47:1300–1306Crossref, Medline, Google Scholar
40 Inouye SK: The dilemma of delirium's clinical and research controversies regarding diagnosis and evaluation of delirium in hospitalized elderly medical patients. Am J Med 1994; 97:278–288Crossref, Medline, Google Scholar
41 Trzepacz PT: Update on Neuropathogenesis of delirium. Dement Geriatr Cogn Disord 1999; 10:330–334Crossref, Medline, Google Scholar
42 Nauseida PA, Weiner WJ, Kaplan LR et al: Sleep disruption in the course of chronic Levodopa therapy: An early feature of Levodopa psychosis. Clin Neuropharm 1982; 5:183–194Crossref, Medline, Google Scholar
43 Comella CL, Tanner CM, Ristanovic RK: Polysomnograpic sleep measures in Parkinson’s disease patients with treatment induced hallucinations. Arch Neurol 1993; 34:710–714Google Scholar
44 Arnulf I, Bonnet AM, Damier P, et al. Hallucinations, REM sleep and Parkinson’s disease. A medical hypothesis. Neurol 2000; 55:281–288Crossref, Medline, Google Scholar
45 Schafer D, Greulich W. Effects of parkinsonian medications on sleep. Journal of Neurology 2000; 247:24–27Crossref, Google Scholar
46 Dewey RB, O'Suilleabhain PE: Treatment of drug-induced psychosis with quetiapine and clozapine in Parkinson’s disease. Neurology 2000; 55:1753–1754Crossref, Medline, Google Scholar
47 The Parkinson Study Group: Low-dose clozapine for the treatment of drug induced psychosis in Parkinson’s disease. NEJM 1999; 340:757–763Crossref, Medline, Google Scholar
48 Freidberg G, Zoldan J, Weizman A: Parkinson’s Psychosis Rating Scale: a practical instrument for grading psychosis in Parkinson’s disease. Clin Neuropharm 1998; 21(5):280–284Medline, Google Scholar
49 Wolters EC, Hurwitz TA, Mak E, et al: Clozapine in the treatment of Parkinsonian patients with dopaminomimetic psychosis. Neurology 1990; 40:832–834Crossref, Medline, Google Scholar
50 Overall J, Gorham D: The Brief Psychiatric Rating Scale. Psychol Rep 1962; 10:799–812.Crossref, Google Scholar
51 Andreasen NC. Scale for the Assessment of Positive Symptoms (SAPS). Iowa City; University of Iowa, 1984Google Scholar
52 Guy W (ed). ECDEU. Assessment Manual for Psychopharmacology, revised. (DHEW publication ADM 76–338), Rockville, MD, National Institute of Mental Health, 1976Google Scholar
53 The Parkinson Study Group: Clozapine for the treatment of drug-induced psychosis in Parkinson’s disease: Results of 12 week open label extension in the PSYCLOPS trial. Mov Disord 2001; 16(1):135–139Crossref, Medline, Google Scholar
54 Mohr E, Mendis T, Hildebrand K, et al: Risperidone in the treatment of dopamine-induced psychosis in Parkinson’s disease: An open pilot trial. Mov Disord 2000; 15(6):1230–1237Crossref, Medline, Google Scholar
55 Meco G, Allesandri A, Bonifati V: Risperidone for hallucinations in Levodopa treated Parkinson’s disease patients. Lancet 1994; 343:1370–1371Crossref, Medline, Google Scholar
56 Ellis T, Cudkowicz ME, Sexton PM, et al: Clozapine and risperidone treatment of psychosis in Parkinson’s disease. J Neuropsych Clin Neurosci 2000; 12(3):364–369Link, Google Scholar
57 Workman RH Jr, Orengo CA, Bakey AA, Molinari VA, Kunik ME. The use of risperidone for psychosis and agitation in demented patients with Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1997; 9:594–597Link, Google Scholar
58 Leopold NA. Risperidone treatment of drug-related psychosis in patients with parkinsonism. Mov Disord 2000; 15:301–304Crossref, Medline, Google Scholar
59 Ford B, Lynch T, Greene P: Risperidone in Parkinson’s disease. [letter] Lancet 1994; 344:681Crossref, Medline, Google Scholar
60 Rich SS, Friedman JH, Ott BR: Risperidone versus clozapine in the treatment of psychosis I six patients with Parkinson’s disease and other akinetic rigid syndromes. J Clin Psychiatry 1995; 56:556–559Medline, Google Scholar
61 Wolters EC, Jansen EN, Tuynman-Qua, HG et al: Olanzapine in the treatment of dopaminomimetic psychosis in patients with Parkinson’s disease. Neurology 1996; 47:1085–1087Crossref, Medline, Google Scholar
62 Aarsland D, Larsen JP, Lim NG, Tandberg E. Olanzapine for psychosis in patients with Parkinson’s disease with and without dementia. J Neuropsychiatry Clin Neurosci 1999; 11:392–394Link, Google Scholar
63 Friedman JH, Goldstein S: Olanzapine in the treatment of dopaminomimetic psychosis in patients with Parkinson’s disease. Neurology 1998; 50:1195–1196Crossref, Medline, Google Scholar
64 Freidman JH, Goldstein SM, Jacques C: Substituting clozapine for olanzapine in psychiatrically stable Parkinson’s disease patients: Results of an open label pilot trial. Clin Neuropharm 1998; 21:285–288Medline, Google Scholar
65 Goetz CG, Blasucci LM, Leurgans S, et al: Olanzapine and clozapine: Comparative effects on motor functions in hallucinating Parkinson’s disease patients. Neurology 2000; 55:789–794Crossref, Medline, Google Scholar
66 Manson AJ, Schrag A, Lees AJ: Olanzapine for Levodopa induced dyskinesias. Neurology 2000; 55:795–799Crossref, Medline, Google Scholar
67 Jibson MD, Tandon R: New atypical antipsychotic medication. J Psychiatr Res 1998; 32:215–228Crossref, Medline, Google Scholar
68 Maixner SM, Mellow AM, Tandon R: The efficacy, safety and tolerability of antipsychotics in the elderly. J Clin Psych 1999; 60(8):29–41Crossref, Google Scholar
69 Freidman JH, Factor SA: Atypical antipsychotics in the treatment of drug-induced psychosis in Parkinson’s disease. Mov Disord 2000; 15(2):201–211Crossref, Medline, Google Scholar
70 Fernandez HH: Quetiapine for Levodopa-induced psychosis in Parkinson’s disease. Letter. Neurology 2000; 55:899Crossref, Medline, Google Scholar
71 Dewey RB, O'Suilleabhain PE: Treatment of drug-induced psychosis with quetiapine and clozapine in Parkinson’s disease. Neurology 2000; 55:1753–1754Crossref, Medline, Google Scholar
72 Roberts VJ, Juncos JL, Wood, CD et al. Quetiapine for psychosis in patients with Parkinson’s disease. [Abstract]. Presented at the American Psychiatric Association Annual Meeting. May 5–10, 2001, New Orleans, LouisianaGoogle Scholar
73 Brandstaeter D, Lotze J, Spieker S et al: High dose quetiapine in neuroleptic naïve patients with Parkinson’s disease and dopaminergic psychosis (abstract). Mov Disord 2001; 16(1):32Crossref, Google Scholar
74 Reddy S, Factor SA, Molho ES, Feustel PJ. The effect of quetiapine on psychosis and motor function in parkinsonian patients with and without dementia. Mov Disord (published on line), April 2, 2002Google Scholar
75 Sommer BR. Quetiapine-induced extrapyramidal side effects in patients with Parkinson’s disease: case report. J Geriatr Psychiatry Neurol 2001; 14:99–100Crossref, Medline, Google Scholar
76 Eichhorn TE, Brunt E, Oertel WH: Ondansetron treatment of Levodopa psychosis. Neurology 1996; 47:1608–1609Crossref, Medline, Google Scholar
77 Cummings JL: Cholinesterase inhibitors: A new class of psychotropic compounds. Am J Psychiatry 2000; 157(1):4–14Crossref, Medline, Google Scholar
78 Small G, Donohue J, Brooks R: An economic evaluation of donepezil in the treatment of Alzheimer's disease. Clin Ther 1998; 20:838–850Crossref, Medline, Google Scholar
79 Shea C, MacKnight C, Rockwood K: Donepezil for treatment of dementia with Lewy bodies: a case series of nine patients. International Psychogeriatrics 1998; 10(3):229–238Crossref, Medline, Google Scholar
80 McKeith I, Delser T, Spano P, et al: Efficacy of rivastigmine in dementia with Lewy bodies: a randomized, double-blind placebo-controlled international study. Lancet 2000; 356:2031–2036Crossref, Medline, Google Scholar
81 Richard IH; Justus AW, Greig N et al: Rivastigmine-induced worsening of motor function and mood in a patient with Parkinson’s disease (abstract). Mov Disord 2001; 16(1):33–34Crossref, Medline, Google Scholar
82 Factor SA, Molho ES, Brown DL: Combined clozapine and electroconvulsive therapy for the treatment of drug induced psychosis in Parkinson’s disease. J Neuropsych 1995; 7(3):304–307Link, Google Scholar
83 Figiel GS, Hassen MA, Zorumski C, et al: ECT-induced delirium in depressed patients with Parkinson’s disease. J Neuropsychiatry Clin Neurosci 1991; 3:405–411Link, Google Scholar
84 Martin M, Figiel G, Mattingly G, et al: ECT-induced interictal delirium in patients with a history of CVA. J Geriatr Psychiatry Neurol 1992; 5:149–155Crossref, Medline, Google Scholar
85 Sobin C, Prudic J, Devanand DP, et al: Who responds to Electroconvulsive therapy? Br J Psychiatry 1995; 169:322–328Crossref, Google Scholar