The American Neuropsychiatric Association
Abstract
The author reviews the history, accomplishments, and goals of the American Neuropsychiatric Association on the occasion of the tenth anniversary of its founding.
The American Neuropsychiatric Association (ANPA) was officially founded in 1988, and we now celebrate the 10th anniversary of this youthful yet remarkably successful organization. This anniversary also provides an opportunity to review the Association's brief history, celebrate its many accomplishments, and look forward into the next millennium to opportunities for its continued success.
For this historical review I relied on many sources of information, including as many formal and informal communications from ANPA as could be found, as well as interviews with ANPA membership, including past and present leaders. Records are relatively scarce from the early years of the Association but have improved dramatically in more recent years.
THE EARLY YEARS (1987–1993)
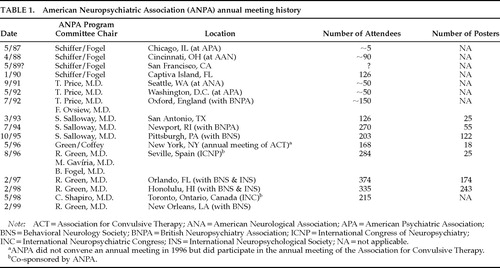
ANPA was the brainchild of two neuropsychiatrists, Barry Fogel, M.D., and Randolph B. Schiffer, M.D. In the late 1980s, Barry Fogel was Director of Adult Psychiatric Services at Rhode Island Hospital. Randy Schiffer was Associate Professor of Neurology and Psychiatry at the University of Rochester School of Medicine, Rochester, New York. Fogel and Schiffer had dreamed for many years about forming an organization of professionals interested in brain–behavior relations, with a particular focus on the behavioral and psychiatric symptoms that occur in some persons with brain disease or dysfunction. Their very first effort at convening such a group took place in early May 1987, in Chicago, during the annual meeting of the American Psychiatric Association (APA). (Table 1 provides a chronology of the ANPA annual meetings.) Drs. Schiffer and Fogel had obtained from the American Board of Psychiatry and Neurology (ABPN) a list of physicians with dual certification in psychiatry and neurology and had invited all of them to the meeting. Schiffer and Fogel hosted a reception with open bar and hors d'oeuvres, but reportedly only about five people attended. Notable among the attendees were two pioneering neuropsychiatrists, Marshall Folstein, M.D., and Max Fink, M.D.; both strongly endorsed the notion of an organization of neuropsychiatrists. Undiscouraged by this inauspicious start, they vowed to try again next year, but this time with a better focus on planning and marketing. It is notable that the chosen acronym for the Association at that time was ANA.
The second meeting of ANPA took place on April 18, 1988, at the Hyatt Regency Hotel in Cincinnati, which was hosting the annual meeting of the American Academy of Neurology (AAN). Dr. Michael Trimble, neuropsychiatrist from Queen Square Hospital, London, gave the keynote address on the topic ”Neuropsychiatry or Behavioral Neurology?” In a newsletter to prospective members mailed May 13, 1988, Dr. Schiffer described that meeting: “There was standing room only and discussion was lively and heated at the conclusion of the lecture. Consultations were held with senior neurologists and behavioral neurologists after the meeting concerning their recommendations about the future of organizations such as ours.” Other notables who attended the meeting included Daniel Weinberger, M.D., of the National Institute of Mental Health, and Janice Stevens, M.D.
In the following month, during the annual meeting of the APA in Montreal, Drs. Schiffer and Fogel held a series of consultative meetings with psychiatrists and neuropsychiatrists from across the United States and Canada, as well as with senior leaders within the APA. As a result of these deliberations, they were emboldened to move forward to formally establish the ANPA. In the May 13, 1988, newsletter described above, Dr. Schiffer made the announcement: ”It is Barry's and my judgment after these discussions that we should go ahead and formally establish the organization, issue bylaws, and formalize the membership, including the charging of dues.” The criteria listed for membership included “…some demonstrated commitment to scholarship, education, or practice in the area of neuropsychiatry. Although we expect that physicians with dual training in psychiatry and neurology will make a natural constituency for the organization, it certainly seems that there are men and women with other training backgrounds who would add much to the organization should they choose to join.” To identify prospective members, Fogel and Schiffer undertook a formal search for physicians with dual board certification in psychiatry and neurology since 1960; 86 such physicians were identified, and their professional activities and opinions were summarized in an interesting article that was later published by Fogel and Schiffer in The Journal of Neuropsychiatry and Clinical Neurosciences (JNCN).1
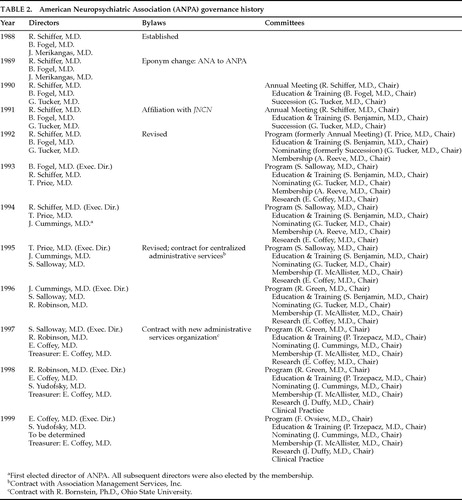
Planning for the Association began in earnest, and on August 31, 1988, Dr. Schiffer sent a second mailing to prospective members, announcing: ”We have with some trepidation made the ANA legitimate!” Their enthusiasm was palpable. The brief letter indicated that the three initial directors of the Association would be Dr. Schiffer, Dr. Fogel, and James Merikangas, M.D., a neuropsychiatrist in private practice in Connecticut. The mailing included a membership application requesting name, address, academic or clinical appointments, and a summary of education and professional training. The membership application fee was $75, $25 for junior members (in training). A set of bylaws was also included, which set forth issues regarding name and purpose, membership, dues and finances, governance, meetings, and amendments to the bylaws. It is of interest that the bylaws defined neuropsychiatry as “a medical specialty committed to better understanding links between neuroscience and behavior, and to the care of individuals with neurologically based behavioral disturbances” and set as the Association's goal the furthering of ”clinical care, education, and research matters relevant to the field of neuropsychiatry.”
The following year, 1989, Dr. Schiffer sent a newsletter on February 28 announcing that the eponym for the Association had been changed from ANA to ANPA to avoid confusion of the former with a more established organization, the American Neurological Association. (It is curious that in this issue had not been raised earlier given the many neurologists involved in the formation of ANPA.) That same newsletter also announced ANPA's next meeting, to occur in May in association with the APA annual meeting in San Francisco. (I can find no information on this ANPA meeting.) Dr. Schiffer also reported that the directors had made a decision to move all future annual meetings “out of the administrative structure of the large neurological and psychiatric organizations,” mainly to establish the ”independent character of the organization” and also to avoid administrative and scheduling difficulties in competing with the larger organizations. Plans were announced for such an independent meeting in Florida for January of the following year.
A second brief newsletter from Dr. Schiffer on July 26, 1989, confirmed a meeting on Captiva Island for January 1990. More important, that newsletter asked the membership for feedback on two questions: 1) should ANPA maintain independent annual meetings or continue efforts to integrate with APA and AAN annual meetings?, and 2) should ANPA affiliate with one of the new neuropsychiatric journals? Both issues were seen by the directors as critical to the future success of the association.
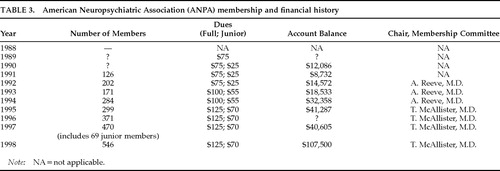
The first independent meeting of ANPA did indeed occur on South Seas Plantation, Captiva Island, Florida, January 25–27, 1990, and its success helped launch the association. An estimated 126 people attended (Table 1). The program focused on “Depression and Neurologic Disease,” and the proceedings were later published in Neuropsychiatry, Neuropsychology, and Behavioral Neurology.2 The meeting's thematic format and its focus on plenary sessions set the template for future meetings. Important decisions regarding governance of the Association were also made during that meeting (Table 2). Dr. Jim Merikangas retired from the directorship and was replaced by Gary Tucker, M.D., Chair of Psychiatry at the University of Washington. This appointment was significant in that it marked the first time that a chair of a major academic department was directly involved in leadership of the association. Three standing committees were established, each chaired by one of the three directors: Annual Meeting Committee (Dr. Schiffer, chair), Education and Training Committee (Dr. Fogel, chair), and Succession Committee (Dr. Tucker, chair). An ad hoc committee was also convened under the leadership of Fred Ovsiew, M.D. (University of Chicago) to begin planning for a joint international meeting with the British Neuropsychiatry Association (BNPA). It was agreed that dues would remain at $75, but no records exist of any discussion of the association's budget. The issue of journal affiliation was discussed extensively. In a follow-up newsletter dated September 13, Dr. Schiffer updated members on the status of this issue as well as the activity of the four committees. The ANPA ended the year with a financial balance of $12,086 (Table 3).
The following year was an important one in terms of growth of the Association. In a February 18, 1991, newsletter Dr. Schiffer announced that the directors had chosen The Journal of Neuropsychiatry and Clinical Neurosciences (Stuart C. Yudofsky, M.D., Editor; American Psychiatric Press, Inc.) as the official journal of the association. Dr. Schiffer noted that ”the feedback from the membership was slanted somewhat in favor of [this journal], but there was a substantial minority of opinion which was respectful and positive towards Dr. [Michael] Taylor's journal, Neuropsychiatry, Neuropsychology and Behavioral Neurology.” In an editorial in the summer issue of JNCN,3 Fogel, Schiffer, and Tucker celebrated this decision and noted that membership in the organization would now include a subscription to JNCN. Each issue of the journal would include information about ANPA business and meeting proceedings. More important, they pointed out that the affiliation represented a mutually beneficial partnership: the association would help JNCN to maintain the distinctive perspective of neuropsychiatry, and JNCN would help ANPA broaden its perspective to include a wider audience of “general psychiatrists, neurologists, psychologists, and others with an interest in contemporary neuropsychiatric developments.”
ANPA held its third annual meeting (Table 1) on September 29, 1991, in Seattle, which was also hosting the ANA annual meeting. (Apparently ANPA was still ambivalent about breaking away entirely from associating with the larger neurology and psychiatry organizations). The program was organized by the new chair of the Program Committee, Trevor R. P. Price, M.D. (Chair of the Department of Psychiatry, Allegheny General Hospital, Pittsburgh, PA). The meeting had about 75 attendees and featured a morning session on ”Educational Issues in Neuropsychiatry” and an afternoon session on “Neuroimaging and Behavior: Neuropsychiatric Applications of Same to the Newer Brain Imaging Techniques.” Dr. Tucker, one of the directors of ANPA, gave the after-dinner lecture on the topic ”Is Neuropsychiatry a Subspecialty?” One important outcome of the morning session was a draft document specifying learning objectives in neuropsychiatry for residents in psychiatry. This draft was prepared by the ANPA Education Committee, then chaired by Sheldon Benjamin, M.D. (Assistant Professor of Psychiatry and Neurology, University of Massachusetts). The document outlined necessary skills in neuropsychiatric evaluation (theory and technique), neuropsychiatric symptoms and syndromes, and neuropsychiatric therapeutics. This document was the first tangible signal of ANPA's desire to make an impact on the education and training of future clinicians. By the fall of 1991, membership in ANPA was 177, 14 of whom were members-in-training. The year-end account balance for ANPA was $8,732 (Table 3).
In January 1992, Dr. Schiffer sent a short letter to ANPA members requesting dues payment (still $75, $25 for junior members) and announcing that membership now stood at 197. That mailing also included the first listing of active members, their addresses, and their practice types. The latter revealed some interesting insights into the membership in those early years: 40% indicated that their practice type was psychiatry, 17% neurology, 15% both psychiatry and neurology, 6% psychology/neuropsychology, 5% other (pediatrics, neurosurgery, emergency medicine, geriatrics), and 15% no response. The majority of members (74%) lived in the eastern United States.
ANPA held its fourth annual meeting in Washington, DC, on May 3, 1992 (Dr. Price, program chair) and featured a symposium on “Medial Temporal Lobe and Neuropsychiatric Illness.” The after-dinner keynote address was given at the Cosmos Club (Richard Restak, M.D., host) by neuropsychiatrist Stuart C. Yudofsky, M.D., then Chair of Psychiatry at University of Chicago Medical Center. ANPA also sponsored an exciting symposium on ”Limbic Disorders” at the APA annual meeting, which was being held concurrently in Washington.
In July of 1992, ANPA held its first international meeting, this in conjunction with BNPA, in Oxford, England. Approximately 150 people attended. Platform sessions focused on the topics of paroxysmal disorders, head injury, and U.S. versus British views on “What is neuropsychiatry?” Case discussions highlighted interesting differences in practice style between American and British clinicians, with the former being more aggressive neuropharmacologists while the latter tended to hospitalize patients for much longer periods of time and undertake more extensive diagnostic evaluations. Proceedings were published in Journal of Neurology, Neurosurgery and Psychiatry.4 This joint meeting initiated numerous transatlantic relationships that have since benefited both organizations.
In the fall of 1992, the ANPA membership voted to ratify revisions to the bylaws. In addition to some minor wording changes, these revisions included formation of two new standing committees, the Membership Committee (to be chaired by Alison Reeve, M.D., University of New Mexico) charged with increasing the membership of ANPA, and the Nominating Committee (to be chaired by the outgoing director, Dr. Tucker) charged with establishing recommendations for candidates for directors and committee chairs (Table 2). In addition, beginning in 1994 directors would now be elected to 3-year terms, in the last year of which each would serve as executive director. The formation of the Nominating Committee signaled that ANPA had now matured from a benevolent oligarchy to a truly democratic association, a transition that was all the more impressive because it was initiated by the leaders themselves.
In January 1993, Dr. Fogel became the first executive director of ANPA, Dr. Schiffer continued as director, and Trevor R.P. Price, M.D. (former chair of the Program Committee) was appointed the fifth director, succeeding outgoing director Gary Tucker, M.D., who became chair of the Nominating Committee. Dr. Price was the second Chair of Psychiatry to serve as a director of the association.
It is said that ”success carries its price,” and in 1993 dues in ANPA were increased to $100, $55 for members-in-training (Table 3). The increase was necessary in large part to offset the cost of sponsorship of JNCN. The fifth annual meeting was held in San Antonio, March 26–28, 1993, and marked a turning point for the Program Committee (now chaired by Stephen Salloway, M.D., Brown University) in terms of planning, scope, and quality of the annual meeting (Table 1). The meeting format consisted of invited lectures, symposia (“Organic Personality Syndromes,” “Neuropsychiatric Aspects of Aging”), after-dinner addresses by director Barry Fogel, M.D. (“Neuropsychiatry in the Era of Managed Care”) and Jeffrey L. Cummings, M.D. (”Von Economo, Freud, and the Lessons of Encephalitis Lethargica”), and, for the first time, a scientific poster session, comprising 25 selected poster presentations on a wide variety of topics. The proceedings and abstracts from the meeting were published in JNCN.5 Approximately 126 participants attended the meeting.
During the business meeting, it was reported that membership had climbed to 235. An ad hoc Committee on Research (chaired by C. Edward Coffey, M.D., Professor of Psychiatry and of Neurology, Allegheny Neuropsychiatric Institute, Pittsburgh, PA) was appointed and charged with developing and leading a research mission and vision for the association. In keeping with Dr. Fogel's presentation on managed care, the directors also appointed a task force on reimbursement (chaired by James Schuster, M.D., Allegheny General Hospital, Pittsburgh, PA). By year's end, the financial account balance was $18,533 (including net revenue for 1993 of $3,961; Table 3).
In six short years, Schiffer and Fogel's vision had become a reality. Clinicians and scientists interested in neuropsychiatry now had their own organization, which was affiliated with a prestigious journal and which produced superb annual scientific meetings. Membership in the association now totaled approximately 200, and formal mechanisms had been established to increase the size of that membership. Revenue from the growth in membership had helped to stabilize the association financially. An effective governance structure had been implemented that involved the members in important activities including education, research, membership, planning of the annual program, and the annual election of a new director.
GROWTH, CONSOLIDATION AND LEADERSHIP IN NEUROPSYCHIATRY (1994–1999)
The next five years marked an important period of growth, consolidation, and leadership in neuropsychiatry for the ANPA.
In 1994, Jeffrey L. Cummings, M.D. (Professor of Neurology and of Psychiatry, UCLA) became the first elected director of ANPA, beginning a 3-year term. (As noted above, directors had previously been appointed by the leadership; Table 2). Dr. Cummings joined Dr. Schiffer, who succeeded Dr. Fogel as executive director, and Dr. Price, who began his second year as director. Dr. Price also began to assume day-to-day administrative responsibilities for the association, a task that Dr. Schiffer had shouldered since ANPA's inception. Outgoing director Fogel joined Tucker on the Nominating Committee.
The sixth annual meeting was held July 21–24, 1994, in Newport, Rhode Island, in joint session with the BNPA (Table 1). Approximately 270 participants attended the meeting, which focused on the theme of “Subcortical Disease in Neuropsychiatry.” The program was ambitious, featuring 32 presentations from platform sessions and symposia, as well as 53 selected scientific poster presentations. Proceedings were published in JNCN.6 Evening lectures were provided by ANPA executive director Schiffer and by BNPA Chair Maria Ron, M.D. Noted neuroscientist Joseph Coyle, M.D., Professor and Chair of Psychiatry at Harvard University, delivered a fine after-dinner presentation at Hammersmith Farm on the topic ”Neuropsychiatry in the 21st Century.”
ANPA committees were becoming increasingly active. The Education Committee (chaired by Dr. Benjamin) began work on securing added qualifications in neuropsychiatry from the American Board of Psychiatry and Neurology (project led by Jeffrey L. Cummings, M.D., and conducted in partnership with the Behavioral Neurology Society [BNS]) and continued its efforts to develop guidelines for training in neuropsychiatry. The AAN had recently granted “Section” status to the BNS. The ANPA also petitioned the APA for appointment of a presidential task force on neuropsychiatry, with the intent of strengthening educational and clinical efforts in neuropsychiatry. To this end, ANPA began formal sponsorship of educational activities at APA annual meetings, including an annual course, “Advances in Neuropsychiatry,” directed by Drs. Coffey and Cummings. The request for a task force was later denied by APA. The Committee on Research (chaired by Dr. Coffey) initiated efforts to facilitate research among ANPA members and undertook a survey of ANPA and BNPA membership to ascertain the extent to which clinical outcomes were formally assessed within neuropsychiatric practice. Liaison with JNCN was also strengthened when its editor, Dr. Yudofsky, determined that all ANPA committee chairs would be appointed to its editorial board. In July the account balance was $32,358; 284 members belonged to ANPA in 1994 (Table 3).
In 1995, Dr. Price succeeded Dr. Schiffer as executive director, Dr. Cummings began his second year as director, and Stephen Salloway, M.D. (Director of Neurology at Butler Hospital, Providence RI, and chair of ANPA's Scientific Program Committee) was elected to a 3-year term as director (Table 2). Recognizing that administration of a growing association required full-time attention, the directors contracted with Association Management Services Inc. (AMS), Prairie Village, Kansas, to assume responsibility for day-to-day administrative operations of the association. The association was incorporated as a not-for-profit organization registered in Kansas, and new bylaws were drafted and ratified later that year. This change in central office was officially announced in an April newsletter to members, which also published the program for the annual meeting later that year. In addition, the directors indicated that membership growth would be a top priority for 1995.
The seventh annual meeting was held October 12–15, 1995, in Pittsburgh, for the first time in conjunction with the BNS (Table 1). The 4-day program was entitled ”Advances in Neuropsychiatry and Behavioral Neurology” and consisted of 5 platform sessions and 122 scientific poster presentations (a 57% increase from the previous year). The after-dinner keynote address was delivered by the late Frank Benson, M.D., on the topic “The Future of Neuropsychiatry and Behavioral Neurology.” The meeting was attended by 203 participants, and 6 junior members received the first Young Investigator Awards presented by the association. Barry Fogel, M.D., was awarded the association's first Distinguished Service Award for his leadership of the association. Proceedings from the meeting were published in JNCN.7
ANPA committees remained very productive. The Reimbursement Task Force (chaired by Dr. Schuster) initiated planning for an affiliation of ANPA with the Institute of Behavioral Healthcare, with a goal of assisting the association in its relations with managed care. Thomas W. McAllister, M.D. (Director, Section of Neuropsychiatry, Dartmouth Medical School) succeeded Dr. Reeve as chair of the Membership Committee (Table 2). The Education Committee (Dr. Benjamin, chair) published the first Directory of Training Programs in Neuropsychiatry and Behavioral Neurology and continued its efforts to petition the ABPN for Added Qualifications for Neuropsychiatry and Behavioral Neurology. This latter initiative was meeting with stiff resistance from APA and ABPN, and to a lesser extent from the AAN, all of whom expressed concerns about designating new subspecialties in an era of anxiety about oversupply of medical specialists. The Research Committee (chaired by Dr. Coffey) completed a survey of ANPA and BNPA membership regarding use of formal outcome assessment in neuropsychiatric practice. The results, which were presented at the Pittsburgh meeting and later published in JNCN,8 indicated that although respondents endorsed the practice of outcome assessment, formal diagnostic evaluations and outcome measures were rarely applied consistently to the broad range of neuropsychiatric conditions encountered clinically. The association continued to strengthen its financial status, with a balance of $41,287 in October. In 1995 membership increased by 25%, to 299 (Table 3).
In 1996, Dr. Cummings succeeded Dr. Price as executive director. Of note, during this same year Cummings also served as President of the BNS, further strengthening the affiliation between the two organizations. Dr. Salloway began his second year as director, and Robert G. Robinson, M.D., Chair of Psychiatry at the University of Iowa, was elected director. (Dr. Robinson was the third Chair of Psychiatry to hold this office.) Outgoing director Price joined the Nominating Committee. Dr. Cummings continued to lead the effort for Added Qualifications in Neuropsychiatry, yet despite his considerable energy, patience, and charm, the effort still encountered major resistance.
Robert C. Green, M.D. (Associate Professor of Neurology, Emory University School of Medicine, Atlanta, GA), succeeded Dr. Salloway as chair of the Scientific Program Committee (Table 2). No formal annual meeting was held in 1996, since the 1995 meeting had taken place in October of 1995 and the 1997 meeting was scheduled for February. However, ANPA did participate in the annual meeting of the Association for Convulsive Therapy (ACT), which took place in May in New York (Table 1). The ANPA Research Committee chair, Dr. Coffey, was also Scientific Program chair for ACT. The theme of that meeting was ”Electricity and Behavior,” and it highlighted the important historical and neurobiologic linkages that exist between electroconvulsive therapy, epilepsy, and neuropsychiatry. Proceedings were published in Convulsive Therapy.9 In August, ANPA also cosponsored the first meeting of the International Congress of Neuropsychiatry in Seville, Spain, which was hosting the World Congress of Psychiatry. That meeting featured plenary and poster sessions on brain imaging, frontal-limbic-subcortical systems, and disorders of cognitive impairment. Dr. Cummings gave the plenary address when invited speaker Alwyn Lishman, M.D., could not attend.
In July of 1996 the ANPA Program Committee (chaired by Dr. Green) surveyed the membership on a variety of issues pertinent to the annual meeting. Approximately half of the members responded. A large majority of respondents strongly endorsed the quality of previous scientific programs, as well as the balance of scientific and clinical presentations. Respondents voiced strong support for holding the meeting at the same time each year, particularly in a warm climate during winter. The results also provided some interesting insights into the membership. The majority (85%) of respondents were male, with a median age range of 40–49 years. Most respondents (88%) held M.D. degrees, and 49% held Ph.D.s. The majority (70%) were actively involved in the management of neuropsychiatric disorders on a regular basis, with 61% practicing in a university setting and 34% in private practice.
The Research Committee (chaired by Dr. Coffey) continued its work on the clinical science of neuropsychiatry. In response to its previous survey indicating that 58% of respondents employed formal assessment of cognitive status, the committee (in a project led by Paul Malloy, Ph.D.) undertook a literature review of the scientific data supporting the use of cognitive screening measures in neuropsychiatry (see below).
The aggressive membership drive undertaken by the Membership Committee (chaired by Dr. McAllister) was yielding good results: membership in 1996 grew by 24%, to 371 (Table 3). An interesting footnote: the Membership Committee was apparently the first to make use of a logo (Figure 1) for ANPA, doing so in a July 1996 mailing. The logo also appeared on a July 1997 mailing, but not subsequently.
The next year, 1997, marked the first in which all three directors of ANPA had been elected by the membership (Table 2). Dr. Salloway succeeded Dr. Cummings as executive director; Dr. Robinson began his second year as director; and C. Edward Coffey, M.D., Professor and Chair of Psychiatry at Henry Ford Health System (and chair of the ANPA Committee on Research) was elected to a 3-year term. Outgoing director Cummings joined the Nominating Committee. Dissatisfied with the management services provided by AMS, the directors quickly implemented a new contract with Robert Bornstein, Ph.D. (Ohio State University) to provide the administrative support for the association. (Bornstein had for many years provided a similar service for the International Neuropsychological Society [INS].) To more effectively manage the increasingly complex finances of the association, the position of Treasurer was established, and Dr. Coffey was appointed its first occupant.
The annual meeting was held February 2–4, 1997, in Orlando, Florida, with the BNS and in conjunction with the INS (Table 1). The program was a major success in terms of attendance (374, the largest ever), participation (174 scientific posters), and scientific breadth and quality. Platform sessions included the evolution of functional imaging in neuropsychiatry, pediatric neuropsychiatry, the aging brain, and the neuropsychiatry of mild head injury. Special presentations were made by Steven Suomi, Ph.D. (“Uptight, Laid Back and Jumpy Monkeys: Individual Differences in Biobehavioral Development”), Sandra Weintraub, Ph.D. (”Neuropsychological Consultation for Neuropsychiatry and Behavioral Neurology”), Richard Mayeux, M.D. (“Neuropsychiatry and Behavioral Neurology in the Molecular Era”), Stephen Hyman, M.D. (discussant), and Jeffrey L. Cummings, M.D. (”Neuropsychology, Neuropsychiatry, and Behavioral Neurology: Common Goals and Uncommon Challenges”). Dr. Randolph B. Schiffer was presented the Distinguished Service Award for his service to ANPA as well as his contributions to the field of neuropsychiatry. Young Investigator Awards were again presented to 5 junior members. Proceedings of the meeting were published in JNCN.10
In July 1997, ANPA also participated in the third joint meeting with the BNPA, this time in Cambridge, England (Fred Ovsiew, M.D., program co-organizer). The meeting featured two major themes: “Frontosubcortical Circuits” and ”Emotion, Reward and Violence.” Proceedings were published in The Journal of Neurology, Neurosurgery and Psychiatry.11
Leadership of the Education Committee changed in 1997, with Paula Trzepacz, M.D. (Professor of Psychiatry and Neurology, University of Mississippi School of Medicine) succeeding Dr. Sheldon Benjamin (Table 2). The committee, in partnership with BNS, continued to encounter resistance in its efforts to press for certification in Neuropsychiatry and Behavioral Neurology. The APA was discouraging further “subspecialization” and declined to review the application. The ABPN agreed to review the application if it was sponsored by the AAN, but AAN had requested substantial changes in the application. After re-review of the proposal, AAN denied support. The committee finally concluded that approval by ABPN was unlikely and therefore began to focus its efforts on ”internal certification.”
The Research Committee (chaired by Dr. Coffey) published its research findings on use of cognitive screening instruments in neuropsychiatry (Paul Malloy, Ph.D., project leader).12 That report found that the Mini-Mental State Examination (MMSE) had widespread popularity, was easy to use, and was supported by a large body of research demonstrating its sensitivity to common neuropsychiatric disorders. The committee recommended that clinicians who employ the MMSE use it as a minimum screening for cognitive dysfunction, employ age- and education-normative corrections, and supplement the MMSE with specific measures of spatial function, delayed memory, and executive abilities. The committee also began work on two other important projects: “The Clinician-Scientist in Neuropsychiatry” (Jeffrey L. Cummings, M.D., project leader) and ”Pharmacologic Efficacy in Neuropsychiatry” (Teresa A. Rummans, M.D., project leader).
The Membership Committee (chaired by Dr. McAllister) enjoyed a banner year in 1997, as membership increased a remarkable 27%, to 470 members (Table 3). The organization remained stable financially with a year-end account balance of approximately $40,605. Finally, ANPA joined the electronic age with the launch of its web site, www.neuropsychiatry.com, designed and maintained by Dr. Paul Malloy.
In 1998, Dr. Robinson succeeded Dr. Salloway as executive director, Dr. Coffey began his second year as director (and continued as treasurer), and Stuart C. Yudofsky, M.D. (Professor and Chair of Psychiatry and Behavioral Sciences, Baylor College of Medicine) was elected to a 3-year term as director. With the election of Dr. Yudofsky, ANPA was led for the first time by three neuropsychiatrists each of whom was a Chair of Psychiatry at a major academic institution.
The annual meeting was held February 1–3, 1998, in Honolulu, Hawaii, again with the BNS and in conjunction with the INS (Table 1). The meeting (and spectacular weather and scenery) were enjoyed by 335 attendees, with the largest-ever number of scientific posters (n=243). Platform sessions featured vascular dementia, movement disorders, repetitive transcranial magnetic stimulation, and neurosurgical treatment. Special presentations were made by M.-Marsel Mesulam, M.D. (“Hemispheric Dominance and Neural Networks in Spatial Awareness”), Christopher G. Goetz, M.D. (”Charcot and Neuropsychiatry”), Sheldon Benjamin, M.D. (“Training Careers in Neuropsychiatry”), Robert G. Robinson, M.D. (”What it Takes to be a Success in Neuropsychiatry”), and David A. Snowdon, Ph.D. (“Aging and Alzheimer's Disease in Catholic Sisters“). Proceedings were published in JNCN.13 In May 1998, ANPA also partnered with the International Neuropsychiatric Congress to cosponsor its first meeting, held in Toronto during the annual meeting of the APA.
ANPA committee work continued at full pace (Table 2). The Education Committee (chaired by Dr. Trzepacz) continued its development of a process for internal certification in neuropsychiatry (Daniel Kaufer, M.D., project leader). The Research Committee (chaired by Dr. Coffey) published two important reports: ”The Clinician-Scientist in Neuropsychiatry”14 (Jeffrey L. Cummings, M.D., project leader) and ”Neuropsychiatric Correlates and Treatment of Lenticulostriatal Diseases“15 (Edward C. Lauterbach, M.D., project leader). James D. Duffy, M.D. (Director of Consultation-Liaison Psychiatry, Hartford Hospital) succeeded Dr. Coffey as chair of the Research Committee. The Membership Committee continued its aggressive membership drive. Final figures were not available at this writing, but membership increased in 1998, and, reflecting both the membership growth and the newly implemented fiscal management, ANPA's financial status remained solid.
CHALLENGES AND OPPORTUNITIES FOR ANPA IN THE NEW MILLENNIUM
The remarkable success of ANPA during its first decade of existence gives rise to strong optimism about the future of the association. ANPA is growing, and it is supported by an active membership that includes world leaders in the field of neuropsychiatry. The major textbooks in the field of neuropsychiatry are all authored by ANPA members. The leaders of the association are dynamic and committed, and they bring important administrative experience from academic medicine. Committees are producing spectacular annual scientific meetings and are setting an international agenda for education and research in the field of neuropsychiatry. The association is fiscally sound and committed to controlling its costs.
But these are challenging times for medicine. Patients are becoming increasingly well educated about their health care and are demanding open access to a broader range of services at demonstrably higher levels of quality. Purchasers of health care are demanding demonstrably better value. And while the demands for better quality and lower costs are increasing, the revenue for such services is declining—the country cannot continue to spend what it has in the past on health care. The former ”cost-based” economy of health care is giving way very rapidly to a ”price-based“ economy. The challenge, of course, for all of medicine and for neuropsychiatry in particular, is to ”do more with less,” to find ways to add value (improved quality and lower costs) to health care.
ANPA is well positioned to lead the response to these challenges on behalf of neuropsychiatry, but to be successful we will need to understand the issues and focus our resources to address them. Specifically, the following action steps are recommended:
| 1. | ANPA should begin a formal strategic planning process, with a goal to complete the plan in time for discussion and finalization at the 2000 annual meeting. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2. | The strategic planning process should begin with establishment of a clear mission and vision statement for the association. What is our raison d'être and what do we want to become? The strategic plan should include the following:
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
A new publication from the ANPA Research Committee illustrates the challenges that neuropsychiatrists face in demonstrating the value of the health care they provide.16 In that report (which will appear in the next issue of JNCN), Teresa A. Rummans, M.D., and colleagues ask the question, “What treatments are effective in management of psychiatric disturbance in patients with brain disease?” They review the world's literature on controlled pharmacologic treatment studies of psychosis, depression, anxiety, and agitation/aggression in patients with cerebral disorders (e.g., stroke, head injury, Alzheimer's disease, multiple sclerosis, Parkinson's disease, Huntington's disease). Interpretation of their findings rests in part on whether one sees the proverbial glass as half empty or half full. For the pessimists, the report reveals a remarkable paucity of controlled treatment data for many of these common ”bread-and-butter” neuropsychiatric conditions. Furthermore, many of the studies that do exist suggest that active treatment is no more effective than placebo, and certainly more fraught with side effects. For the optimists, there is limited evidence of efficacy for pharmacologic treatment in at least some of the conditions reviewed.
Going forward into the new millennium, our challenge as neuropsychiatrists is to demonstrate that we add value to the care of patients with behavioral disturbances and brain disease. This is a noble mission, and ANPA is in an excellent position to lead the charge. Given the energy, creativity, expertise, and commitment of our membership, I am certain that we will succeed.
ACKNOWLEDGMENTS
The following reviewed earlier versions of this manuscript and provided helpful comments: Jeffrey L. Cummings, M.D., Barry Fogel, M.D., Robert C. Green, M.D., Trevor R. P. Price, M.D., Robert G. Robinson, M.D., Stephen Salloway, M.D., Paula Trzepacz, M.D., Gary Tucker, M.D., and Stuart C. Yudofsky, M.D.
This material will be presented in an address to the membership at the tenth annual meeting of the American Neuropsychiatric Association, January 31–February 2, 1999, New Orleans, LA.

FIGURE 1. The first ANPA logo, apparently designed by AMS, Inc.
 |
 |
 |
1 Fogel BS, Schiffer RB: Defining neuropsychiatry: professional activities and opinions of psychiatrist-neurologists with dual certification. J Neuropsychiatry Clin Neurosci 1989; 1:173–175Link, Google Scholar
2 Fogel BS, Schiffer RB (eds): The neuropsychiatry of depression. Neuropsychiatry Neuropsychol Behav Neurol 1991; 4:1–92Google Scholar
3 Fogel B, Schiffer R, Tucker G: Allies with a common cause: the American Neuropsychiatric Association and The Journal of Neuropsychiatry and Clinical Neurosciences. J Neuropsychiatry Clin Neurosci 1991; 3:241–242Link, Google Scholar
4 Editor: Proceeedings of the joint summer meeting of the British and American Neuropsychiatry Associations, 12–14 July 1992, Oxford. J Neurol Neurosurg Psychiatry 1992; 55:1098–1100Crossref, Medline, Google Scholar
5 American Neuropsychiatric Association: Highlights of the 5th annual meeting, American Neuropsychiatric Association, March 26–28, 1993, San Antonio, Texas. J Neuropsychiatry Clin Neurosci 1993; 5:442–456Link, Google Scholar
6 American Neuropsychiatric Association: Sixth annual meeting, American Neuropsychiatric Association, with the British Neuropsychiatry Association, July 21–24, 1994, Newport, Rhode Island: “Subcortical Disease in Neuropsychiatry,” scientific program abstracts. J Neuropsychiatry Clin Neurosci 1994; 6:297–323Link, Google Scholar
7 American Neuropsychiatric Association: Seventh annual meeting, American Neuropsychiatric Association, in conjunction with the Behavioral Neurology Society, October 12–15, 1995, Pittsburgh, Pennsylvania: “Advances in Neuropsychiatry and Behavioral Neurology,” scientific program abstracts. J Neuropsychiatry Clin Neurosci 1995; 7:391–429Link, Google Scholar
8 ANPA Education Committee: 1995 Directory of Training Programs in Behavioral Neurology and Neuropsychiatry. J Neuropsychiatry Clin Neurosci 1995; 7:557–560Google Scholar
9 Coffey CE: Meeting abstracts for the sixth annual meeting of the Association for Convulsive Therapy. Convuls Ther 1996; 12:63–77Google Scholar
10 American Neuropsychiatric Association: Eighth annual meeting, American Neuropsychiatric Association, a joint meeting with the Behavioral Neurology Society in conjunction with the International Neuropsychological Society, February 2–4, 1997, Orlando, Florida: scientific program. J Neuropsychiatry Clin Neurosci 1997; 9:125–180Link, Google Scholar
11 Ron MA: Proceedings of the joint summer meeting of the British Neuropsychiatric Association and the American Neuropsychiatric Association, Cambridge, 20–22 July 1997. J Neurol Neurosurg Psychiatry 1998; 64:423–425Google Scholar
12 Malloy PF, Cummings JL, Coffey CE, et al: Cognitive screening instruments in neuropsychiatry: a report of the Committee on Research of the American Neuropsychiatric Association. J Neuropsychiatry Clin Neurosci 1997; 9:189–197Link, Google Scholar
13 American Neuropsychiatric Association: Ninth annual meeting, American Neuropsychiatric Association, a joint meeting with the Behavioral Neurology Society in conjunction with the International Neuropsychological Society, February 1–3, 1998, Honolulu, Hawaii: scientific program. J Neuropsychiatry Clin Neurosci 1997; 9:631–706Link, Google Scholar
14 Cummings JL, Coffey CD, Duffy JD, et al: The clinician-scientist in neuropsychiatry: a position statement from the Committee on Research of the American Neuropsychiatric Association. J Neuropsychiatry Clin Neurosci 1998; 10:1–9Link, Google Scholar
15 Lauterbach EC, Cummings JL, Duffy J, et al: Neuropsychiatric correlates and treatment of lenticulostriatal diseases: a review of the literature and overview of research opportunities in Huntington's, Wilson's, and Fahr's diseases. J Neuropsychiatry Clin Neurosci 1998; 10:249–266Link, Google Scholar
16 Rummans TA, Lauterbach EC, Coffey CE, et al: Pharmacologic efficacy in neuropsychiatry: a review of placebo-controlled treatment trials. J Neuropsychiatry Clin Neurosci (in press)Google Scholar